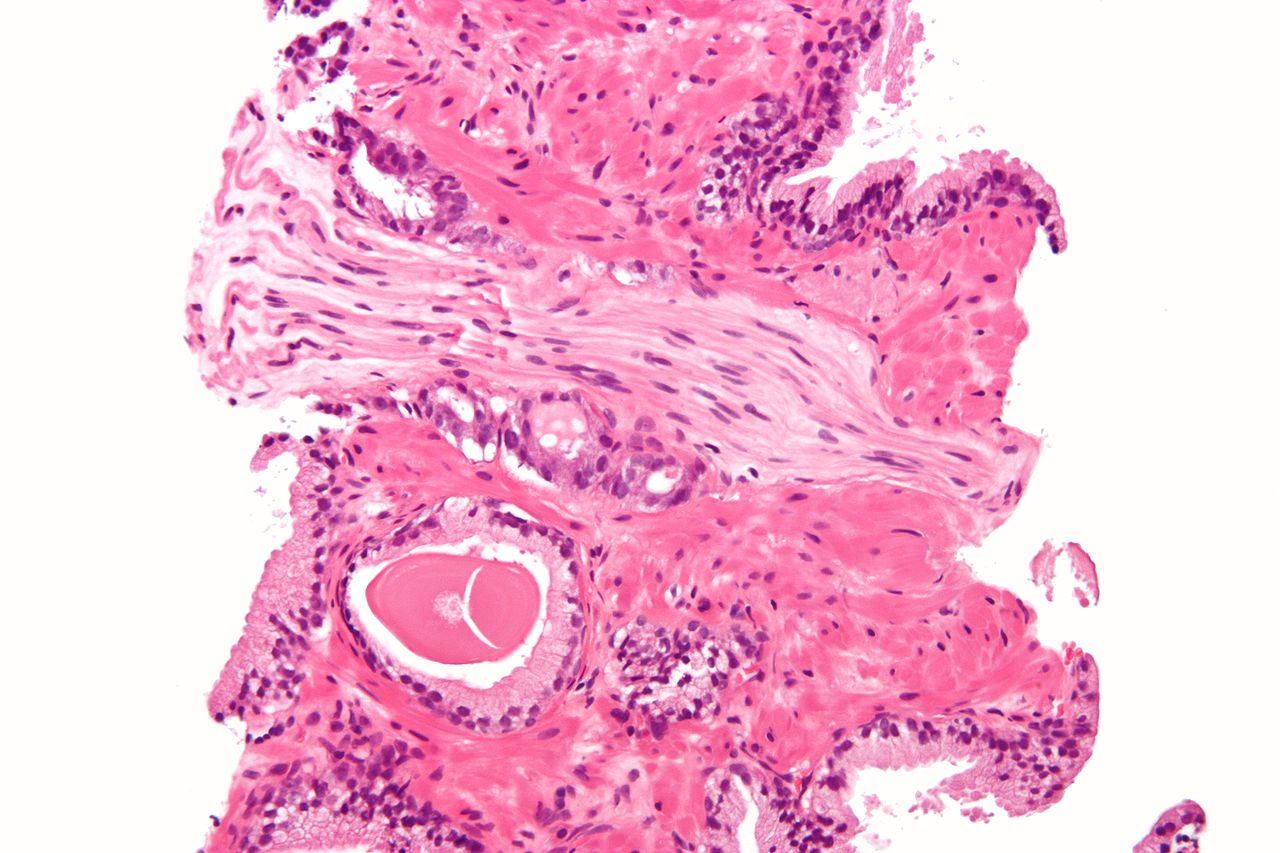
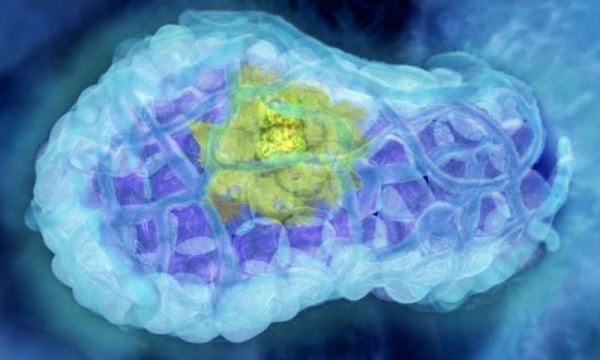
Photomicrograph showing prostate cancer (common adenocarcinoma) with perineural invasion
Cancer cells can grow into the nerves of the gut and use them as pathways for metastasis. How does this happen?
There are several types of perineural invasion when tumor cells:
approach the outer layer of the nerve fiber without its sprouting
penetrate the nerve
grow into the intestinal wall along their own nerve plexuses
Mechanistically, we imagine that the tumor divides, grows and at some point grows into the nerve fibers. In fact, each nerve is surrounded by a sheath of dense collagen and basement membrane. It’s not easy to break this defense.
But the tumor copes with this task. It releases substances that make a hole in the membrane, cancer cells penetrate inside the nerve and spread their metastases further.
Perineural invasion is one of the parameters that is included in the TNM system – the international classification of tumors. The need to describe this parameter appeared recently. Previously, this information could not be specified.
Often, pathologists are asked to additionally describe the nature of the invasion – to clarify whether there is a germination of the tumor into the nerve, or a single tumor cell is simply dangerously close.
Perineural invasion worsens the prognosis of disease-free survival. Moreover, if the tumor grows inside the nerve fiber, this worsens the prognosis by another 20%.
The most incredible thing is that the tumor and the nerves interact with each other. Nerve tissue helps cancer cells grow and grow around themselves, but scientists haven’t figured out why yet.
The tumor also initiates the growth of nervous tissue around itself, which it uses as paths along which it will spread further into the tissues.
In any case, if cancer cells were able to overcome the protective barrier of the nerve, this indicates their aggressiveness. Therefore, it is necessary to start treatment without delay. It will not be easy to cope with metastases, here even chemotherapy is often unable to help.
The parameter perineural invasion is very important. In conjunction with other parameters, it allows you to correctly assess the potential of the tumor to spread over long distances and plan postoperative treatment.
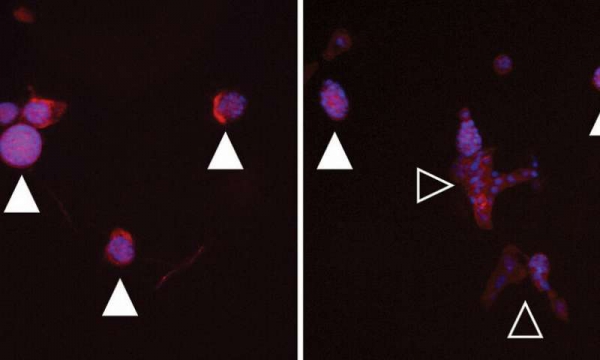
Left: Image of a soft hydrogel with normally developing cell cultures (filled triangles). Right: Image of a stiffened, tumor-like hydrogel with transformed cells (open triangles). Credit: Matt Ondeck and Jesse Placone
A study provides new insight into how the stiffening of breast tissue plays a role in breast cancer development. By examining how mammary cells respond in a stiffness-changing hydrogel, bioengineers at the University of California San Diego discovered that several pathways work together to promote the transformation of breast cells into cancer cells. The work could inspire new approaches to treating patients and inhibiting tumor growth.
The team reported their findings in a paper published online on Feb. 12 in the Proceedings of the National Academy of Sciences (PNAS).
“By dynamically modulating the stiffness of the microenvironment, we can better mimic what happens during the transformation of breast cells to a malignant state in a dish,” said senior author Adam Engler, a professor of bioengineering at the UC San Diego Jacobs School of Engineering.
The study is part of a growing body of research showing that mechanical forces—not just genetic and biochemical signals—play a key role in the development and spread of cancer. In the past, researchers have found that modeling stiff tissue environments in vitro promoted tumor growth.
But these models often do not fully recreate what’s happening in the body because they are static, Engler noted. “Tissue stiffening is a dynamic process. Mammary tissue doesn’t just start out stiff, this is something that develops over time,” said Engler.
So Engler’s approach was to use a material system in which the stiffness could be tuned dynamically while cells are inside, and then see how the cells respond to that change in stiffness.
“We’re trying to mimic the process of fibrosis during the progression of tumor development,” said Jesse Placone, a postdoctoral fellow in Engler’s lab and a co-first author of the study. “As a tumor site forms, the local stiffness of the tissue increases. And by modeling this dynamic stiffness, our system is significantly more representative of what happens in vivo.”
The team used a hydrogel called methacrylated hyaluronic acid, a soft material that can be stiffened to varying degrees with exposure to free radicals and UV light. They first stiffened the hydrogel enough to mimic the stiffness of normal breast tissue. Then, they cultured mammary epithelial cells in the gel. After the cells matured, the gel’s stiffness was increased to that of a breast tumor. The amount of UV exposure required in this step was not enough to harm the cells, the team noted.
They discovered that stiffening triggers multiple pathways that together signal mammary cells to become cancerous. Key players of these pathways include the proteins TWIST1, TGF-beta, SMAD and YAP.
“In a dynamic environment, we found that these different pathways act cooperatively. It’s not enough to inhibit just one of those pathways as was previously shown in studies modeling static, stiff environments,” said Engler. “From a clinical perspective, this suggests that a single drug approach may not work for all patients with breast cancer tumors.”
The team also discovered that a subpopulation of mammary cells do not respond to stiffening. Engler says this is good news for women as fewer cells than previously thought may turn into cancer as a result of the environment alone. Such a result, if it translates to patients, could mean fewer or smaller primary tumors.
The team next plans to explore drug candidates to inhibit the pathways and study their effects on tumor progression. This research was done primarily on genetically controlled cell lines, so the team will follow up with studies on patient-derived cell lines.
Vlastimil Gular’s life took an unwelcome turn a year ago: minor surgery on his vocal cords revealed throat cancer, which led to the loss of his larynx and with it, his voice
Vlastimil Gular’s life took an unwelcome turn a year ago: minor surgery on his vocal cords revealed throat cancer, which led to the loss of his larynx and with it, his voice.
But the 51-year-old father of four is still chatting away using his own voice rather than the tinny timbre of a robot, thanks to an innovative app developed by two Czech universities.
“I find this very useful,” Gular told AFP, using the app to type in what he wanted to say, in his own voice, via a mobile phone.
“I’m not very good at using the voice prosthesis,” he added, pointing at the hole the size of a large coin in his throat.
This small silicon device implanted in the throat allows people to speak by pressing the hole with their fingers to regulate airflow through the prosthesis and so create sound.
But Gular prefers the new hi-tech voice app.
It was developed for patients set to lose their voice due to a laryngectomy, or removal of the larynx, a typical procedure for advanced stages of throat cancer.
The joint project of the University of West Bohemia in Pilsen, Prague’s Charles University and two private companies—CertiCon and SpeechTech—kicked off nearly two years ago.
The technology uses recordings of a patient’s voice to create synthetic speech that can be played on their mobile phones, tablets or laptops via the app.
Jindrich Matousek, an expert on text-to-speech synthesis, heads the project at the University of West Bohemia in Pilsen
Ideally, patients need to record more than 10,000 sentences to provide scientists with enough material to produce their synthetic voice.
“We edit together individual sounds of speech so we need a lot of sentences,” said Jindrich Matousek, an expert on text-to-speech synthesis, speech modelling and acoustics who heads the project at the Pilsen university.
‘A matter of weeks’
But there are drawbacks: patients facing laryngectomies usually have little time or energy to do the recordings in the wake of a diagnosis that requires swift treatment.
“It’s usually a matter of weeks,” said Barbora Repova, a doctor at the Motol University Hospital, working on the project for Charles University.
“The patients also have to tackle issues like their economic situation, their lives are turned upside down, and the last thing they want to do is to make the recording,” she told AFP.
To address these difficulties, scientists came up with a more streamlined method for the app, which is supported by the Technology Agency of the Czech Republic.
Working with fewer sentences—ideally 3,500 but as few as 300—this method uses advanced statistical models such as artificial neural networks.
Working on the project to develop an app to help give throat cancer patients their voice back is doctor Barbora Repova, who represents Charles University
“You use speech models with certain parameters to generate synthesised speech,” said Matousek.
“Having more data is still better, but you can achieve decent quality with less data of a given voice.”
The sentences are carefully selected and individual sounds have to be recorded several times as they are pronounced differently next to different sounds or at the beginning and end of a word or sentence, he added.
So far, the Pilsen university has recorded 10 to 15 patients, according to Matousek.
Besides Czech, the Pilsen scientists have also created synthesised speech samples in English, Russian and Slovak.
‘Baby dinosaurs’
Gular—an upholsterer who lost his job due to his handicap—managed to record 477 sentences over the three weeks between his diagnosis and the operation.
But he was stressed and less than satisfied with the quality of his voice.
Entrepreneur Jana Huttova records sentences to be able to use the app if she loses her voice to minor throat surgery
“Throat cancer patients often suffer from some form of dysphonia (hoarseness) before the surgery, so in combination with a limited speech sample it makes the voice sound unnatural,” said Repova.
In a studio at the Pilsen university meanwhile, entrepreneur Jana Huttova is recording outlandish phrases.
The 34-year-old mother of three faces the risk of losing her voice to minor throat surgery—an operation on her parathyroid gland.
“The Chechens have always preferred a dagger-like Kalashnikov,” she says, reading from the text before her.
“I have small kids and I want them to hear my own voice, not a robot,” Huttova said.
Then she moved on to her next sentence: “We were attacked by a tyrannosaur’s baby dinosaurs.”
Connected to the brain
Matousek believes that in the future, patients will be able to use the app to record their voice at home using a specialised website to guide them through the process.
Jana Huttova, 34, a mother of three, says she is recording phrases for the app because she would want her children to hear her voice, not a robot
And he hopes that one day it will go even further.
“The ultimate vision is a miniature device connected to the brain, to the nerves linked to speech—then patients could control the device with their thoughts,” he said.
This kind of advanced solution is a very long way off, said Repova.
“But look at cochlear implants—40 years ago when they started, we had no idea how it would develop, how widely they would end up being used,” she said, referring to the inner-ear implants used to tackle severe deafness.
“A happy end would be a device implanted in the throat that could talk with the patient’s own voice,” she told AFP.
“It’s realistic: it may not come in a year or even in 10 years, but it’s realistic and we’re on the way.”
A team of researchers from the U.K., Denmark, Poland, the Netherlands and Switzerland has developed a new way to test for cancer—by looking at the size of tumor DNA fragments circulating in the bloodstream. In their paper published in the journal Science Translational Medicine, the group describes their technique and how well it worked when tested on patients with different kinds of cancer. Ellen Heitzer and Michael Speicher, with Medical University of Graz, offer a Focus piece on the work done by the team in the same journal issue.
As Heitzer and Speicher note, human blood contains many small DNA fragments, most of them from white blood cells. But there are instances where other types are introduced, for instance, DNA from a fetus in the blood of pregnant women, or bits of DNA that break loose from cancerous tumors. In this new effort, the researchers discovered that DNA from tumors can be differentiated from other types of DNA in the blood by size—such fragments tend to be smaller than DNA fragments from other sources.
To take advantage of this finding, the researchers carefully studied DNA fragments in the blood from several types of cancer and found they could be classified by size. They then created a new metric of measurement for them based on size. They called it trimmed median absolute deviation from copy number neutrality (t-MAD). The team then tested their approach by introducing DNA fragments into a blood sample and then used a benchtop fluidic device to focus on the DNA fragments, which they assigned a t-MAD rating. Pleased with their findings, they further tested their approach by conducting similar tests with blood from actual cancer patients.
The researchers report that their testing showed the technique to be very reliable—it offered positive results for 94 percent of breast, bowel, ovary, skin and bile duct cancers with a false positive rate of just 2.5 percent. It also proved to be 65 percent accurate in detecting pancreas, kidney and brain cancers.
Heitzer and Speicher point out that there are still some questions regarding the technique, however. Chief among them is whether testing will be as accurate when used in a large multicenter clinical setting.
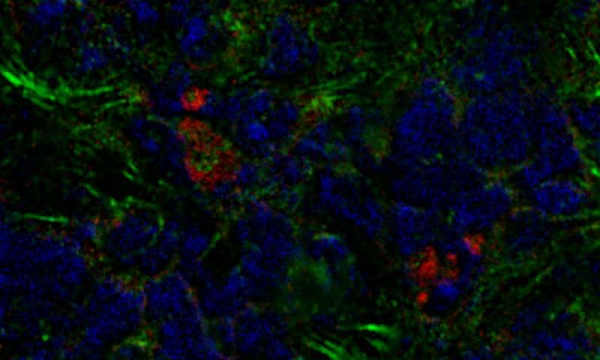
A mouse breast tumor contains bone marrow-derived fibroblasts (red) as well as other cancer-associated fibroblasts (green). Credit: Raz et al., 2018
Researchers in Israel have discovered that breast tumors can boost their growth by recruiting stromal cells originally formed in the bone marrow. The study, which will be published November 23 in the Journal of Experimental Medicine, reveals that the recruitment of bone marrow-derived fibroblasts lowers the odds of surviving breast cancer, but suggests that targeting these cells could be an effective way of treating the disease.
Within solid tumors, cancer cells are surrounded by other cell types that, though not cancerous themselves, boost tumor growth and metastasis. Breast tumors, for example, contain large numbers of fibroblast cells that promote cancer cell proliferation, inflammation, and the formation of new blood vessels to supply the growing tumor with nutrients and oxygen. Many of these cancer-associated fibroblasts are derived from the neighboring breast tissue, but others seem to come from elsewhere in the body.
Neta Erez and colleagues at the Sackler School of Medicine, Tel Aviv University, discovered that, in mice with breast cancer, a significant number of cancer-associated fibroblasts are derived from bone marrow cells called mesenchymal stromal cells (MSCs). The researchers found that breast tumors can recruit MSCs from the bone marrow and cause them to develop into fibroblasts.
These bone marrow-derived fibroblasts are different from other cancer-associated fibroblasts. They lack, for example, a key cell signaling protein called PDGFRα. But bone marrow-derived fibroblasts are particularly effective at stimulating the formation of new blood vessels because they produce large amounts of a protein called clusterin. Tumors containing bone marrow-derived fibroblasts were therefore more vascularized and grew faster than tumors that only contained breast-derived fibroblasts.
Erez and colleagues found that human breast cancers also contain fibroblasts lacking PDGFRα, suggesting that human tumors may also recruit bone marrow-derived cells. Moreover, tumors containing lower levels of PDGFRα tended to be more deadly, suggesting that the recruitment of bone marrow-derived fibroblasts is a crucial step in breast cancer progression.
“Our study shows that the recruitment of bone marrow-derived fibroblasts is important for promoting tumor growth, likely by enhancing blood vessel formation,” Erez says. “Understanding the function of these cancer-associated fibroblasts could form the basis of developing novel therapeutic manipulations that co-target bone marrow-derived fibroblasts as well as the cancer cells themselves.”
When melanoma turns metastatic, it spreads to the brain in more than 40% of patients. A study by Yale Cancer Center researchers published today in the Journal of Clinical Oncology (JCO) shows a checkpoint inhibitor immunotherapy drug has meaningful benefit for these patients. The study is one of the first clinical trials aimed at treating the brain metastases with this type of cancer drug.
“The study treated 23 patients with pembrolizumab, a drug that targets PD-1 proteins on the surface of T cells,” said the study’s lead author, Harriet Kluger, M.D., director of the Specialized Program of Research Excellence (SPORE) in Skin Cancer at YCC and professor of medicine at Yale School of Medicine. “Six of the trial participants (26% of the total) saw their tumors shrink or resolve, and the drug’s toxicity levels were acceptable.”
Importantly, added Kluger, about half of the patients were alive after two years, a rate similar to that of patients in other trials who had metastatic melanoma without brain tumors and were given anti-PD-1 drugs.
“One of the big messages of our study is that patients with metastatic melanoma who had a response to this drug elsewhere in the body also had a response in the brain,” she said. “This suggests that for some patients, metastases can be treated similarly in the brain and the body, particularly if the brain metastases are small and not located in critical sites. However, caution should be taken with this approach, and a multidisciplinary clinical team including close involvement of neurosurgeons and therapeutic radiologists is necessary in case no shrinkage is seen.”
Kluger noted that another recently reported trial for patients with untreated brain melanoma metastases who were given two immunotherapy drugs achieved a significantly higher rate of response. Results published in the New England Journal of Medicine showed a clinical benefit of 57% among 94 patients who were treated with another PD-1 inhibitor plus a checkpoint inhibitor that targets the CTLA-4 protein on the surface of T cells.
Together, these latest clinical findings suggest that melanoma patients with brain metastases should be given a combination of the two types of checkpoint inhibitors, if the patients are healthy enough for this aggressive regimen, Kluger said. Treatment with a PD-1 inhibitor is appropriate if the patients are not so robust or perhaps if the brain tumors are tiny and not producing symptoms of disease, she said.
Until recently, people with brain metastases were typically excluded from clinical trials of novel therapies. One reason, Kluger said, is because researchers found it hard to track which drugs could penetrate the blood-brain barrier (the special vasculature that protects the brain and often keeps out cancer drugs). Clinicians also worried that if the drugs didn’t work, they would lose control of the disease. With improvements in drugs, brain imaging and radiation treatments, researchers now have become more comfortable with starting trials for brain metastases, said Kluger.
Major questions remain, however, about immunotherapy for brain metastases, she noted. Scientists don’t know how well these drugs penetrate the blood-brain barrier, which is disrupted in tumors. Scientists also don’t know whether the drug actually gets into the brain or whether it stimulates immune cells that then enter the brain, Kluger pointed out. Researchers do know that the collection of immune and vascular cells in the area around the tumor and within the tumor, known as the tumor microenvironment, may behave quite differently in the brain than elsewhere in the body, which can change how (and if) a drug works.
The YCC clinicians are following up with another trial that will combine pembrolizumab with bevacizumab, a drug that aims to stop the growth of blood vessels that supply tumors. The hope is that this combination will aid in reducing complications that patients may suffer from radiation before they are given immunotherapy. The investigators expect to release an initial report on the follow-up study in 2019.
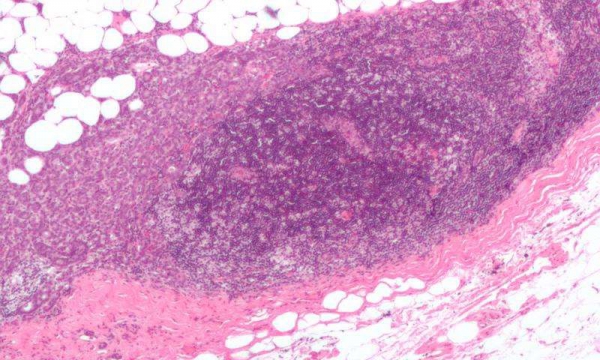
Micrograph showing a lymph node invaded by ductal breast carcinoma, with extension of the tumour beyond the lymph node. Credit: Nephron/Wikipedia
Women who take part in breast screening have a significantly greater benefit from treatments than those who are not screened, according to a study of more than 50,000 women, led in the UK by Queen Mary University of London.
The research, using data from Sweden, finds that women who chose to participate in an organised breast cancer screening programme had a 60 per cent lower risk of dying from breast cancer within 10 years after diagnosis, and a 47 per cent lower risk of dying from breast cancer within 20 years after diagnosis.
The authors say that this benefit occurs because screening detects cancers at an earlier stage, meaning that they respond much better to treatment.
The study was co-authored and funded by the American Cancer Society and appears in the American Cancer Society’s peer-review journal Cancer.
In the UK, mammography screening is offered to all women aged 50-70 through the NHS Breast Screening Programme, with participation rates averaging more than 70 per cent but varying dramatically across the country, with lower rates in poorer, inner-city areas.
Senior author Professor Stephen Duffy from Queen Mary University of London said: “Recent improvements in treatments have led to reduced deaths from breast cancer. However, these new results demonstrate the vital role that screening also has to play, giving women a much greater benefit from modern treatments. We need to ensure that participation in breast screening programmes improves, especially in socio-economically deprived areas.”
The study involved 52,438 women aged 40 to 69 years in the county of Dalarna, Sweden, during 39 years of the screening era (1977-2015). All patients received stage-specific treatment according to the latest national guidelines, irrespective of the mode of detection.
The investigators, led by Laszlo Tabar, M.D., of Falun Central Hospital in Sweden, used a new method to improve the evaluation of the impact of organised mammography screening on death from breast cancer, by calculating the annual incidence of breast cancers causing death within 10 years and within 20 years after breast cancer diagnosis.
Manjeet Rao, Ph.D., of UT Health San Antonio, led a study that showed a small molecule is able to kill a childhood brain cancer called medulloblastoma. The molecule sensitizes the cancer to chemotherapy and radiation, offering hope that in the future oncologists could treat this cancer with far less chemotherapy and radiation. Credit: UT Health San Antonio
Sometimes small things make the biggest differences.
A new study by UT Health San Antonio researchers found that a molecule thousands of times smaller than a gene is able to kill medulloblastoma, the most common childhood brain cancer.
This tiny molecule, named MiR-584-5p, is quite efficient in its action. MiR-584-5p sensitizes the cancer to chemotherapy and radiation, making it plausible to treat the tumors with one-tenth the dose that is currently required, said study senior author Manjeet Rao, Ph.D., associate professor of cell systems and anatomy at UT Health San Antonio and a member of the university’s Greehey Children’s Cancer Research Institute.
“Currently we barrage the brain with radiation and chemo, and patients have poor quality of life,” Dr. Rao said. “Using this molecule, we could dial down those therapies considerably, by 90 percent. That’s exciting.”
MiR-584-5p is at very low levels or absent altogether in medulloblastoma. Increasing it to the amount found in healthy cells robs the cancer of mechanisms it uses to survive, studies show. “This can serve as a potent therapeutic for treating cancer,” Dr. Rao said.
The journal Nature Communications published the findings Oct. 31.
The other excitement about MiR-584-5p is that it is normally present at high levels in brain cells and not so in other tissues, Dr. Rao said. Therefore, when it is used in the brain as therapy to kill tumors, it will have negligible effects on the healthy cells because those cells have seen it before. “They may not treat the molecule as something foreign,” Dr. Rao said. A future therapy based on the molecule should be well-tolerated, he said.
A big challenge for treating brain cancer patients is the inability of cancer drugs to cross the blood-brain barrier, a protective mechanism that holds up brain cancer therapies. Because it is so petite, MiR-584-5p may be able to cross this barrier, which is leaky in some medulloblastoma patients. In the future, Dr. Rao said, the molecule may be delivered using a nanoparticle carrier.
Aside from medulloblastoma, the properties of MiR-584-5p make it an excellent drug candidate for treatment of glioblastoma, an aggressive and lethal adult brain cancer, Dr. Rao said.
A patent on the MiR-584-5p technology has been filed with Dr. Rao and Nourhan Abdelfattah, Ph.D., first author on the paper, listed as inventors. Dr. Abdelfattah completed her doctoral work in the Rao laboratory and is a postdoctoral fellow at Houston Methodist Cancer Center.
A second patent with Dr. Rao as inventor was issued by the U.S. Patent and Trademark Office. Multiple commercialization business models are under review, including a possible start-up company, according to the Office of Technology Commercialization at UT Health San Antonio.
Biomedical animation of a breast tumour Credit: Drew Berry, Walter and Eliza Hall Institute
Melbourne scientists have discovered how tumour development is driven by mutations in the most important gene in preventing cancer, p53.
The research revealed that in the early stages of cancer, mutant p53 ‘tackles’ the normal p53 protein and blocks it from carrying out its protective role. As a result, p53 can no longer activate natural defences against cancer—such as the body’s DNA repair process—increasing the risk of cancer developing.
The research was led by Dr. Brandon Aubrey, Professor Andreas Strasser and Dr. Gemma Kelly together with bioinformaticians Professor Gordon Smyth and Dr. Yunshun Chen. The findings are published in this month’s edition of Genes and Development.
Tackling DNA’s guardian
p53 is known as the ‘guardian of the genome’ due to its role in protecting cells from cancer.
“p53 plays a critical role in many pathways that prevent cancer, such as repairing DNA or killing cells if they have irreparable DNA damage,” Dr. Kelly said.
“Genetic defects in p53 are found in half of all human cancers, but exactly how these changes disrupt p53 function has long been a mystery.”
Dr. Kelly said that cells normally have two copies of the p53 gene in every cell.
“Early during cancer development, one copy of the gene may undergo a sudden and permanent change through mutation, while the other copy of the gene remains normal. This results in the cell making a mixture of normal and mutant versions of the p53 protein.
“We found that the mutant p53 protein can bind to and ‘tackle’ the normal p53 protein, blocking it from performing protective roles such as DNA repair. This makes the cell more likely to undergo further genetic changes that accelerate tumour development.”
The team expected the mutant proteins would block all normal p53 activity, so was surprised to find that only certain p53-dependent pathways were affected.
“The mutant proteins are cunning: while they stop p53 from activating pathways that protect against cancer, they still allow p53 to activate pathways that promote tumour growth. p53’s role in cancer is clearly more complicated than we had expected,” Dr. Kelly said.
A mystery resolved
Professor Strasser said the findings inform a longstanding debate about mutant p53.
“Scientists have been debating how mutant p53 contributes to the development of cancer for decades.
“One camp argues that mutant p53 acts by ‘tackling’ the normal protein and blocking its natural protective roles. The other camp argues that mutant p53 goes ‘rogue’ and performs new roles that promote tumour development.”
“Our work clearly shows that during cancer development, the ‘tackling’ of normal p53 is most significant. This selectively disables certain but not all normal functions of p53,” Professor Strasser said.
Clinical implications
The team is now investigating whether the same is true for established tumours, with important implications for drug treatments.
“Established tumours have often lost the normal copy of their p53 gene and only produce mutant p53 protein,” Dr. Kelly said.
“If mutant p53 acts by tackling normal p53, then it may no longer play a role in established tumours where no normal p53 is produced. This would mean that drugs that block mutant p53 would have no clinical benefit,” she said.
“Conversely, if mutant p53 has new, cancer-promoting activities of its own in established tumours, then a drug that specifically blocks mutant p53 could be beneficial for treating thousands of patients.”
Melanoma in skin biopsy with H&E stain — this case may represent superficial spreading melanoma. Credit: Wikipedia/CC BY-SA 3.0
Melanoma is the leading cause of death from skin cancer. Many patients develop metastatic disease that spreads to other parts of the body. One commonly used targeted therapy for metastatic melanomas works by attacking melanomas with mutations in the BRAF gene that make them susceptible to RAF-inhibiting drugs. However, many cancers quickly become resistant to the treatment. Now researchers at the NCI-designated Sidney Kimmel Cancer Center—Jefferson Health have discovered how one of the mechanisms of that resistance works, a finding that could lead to designing more effective combination therapies.
“The findings give us new clues about how we might combat resistance to this targeted melanoma therapy,” said Andrew Aplin, Ph.D., Associate Director for Basic Research and the Program Leader for Cancer Cell Biology and Signaling (CCBS) at the Sidney Kimmel Cancer Center. The research was published November 6th in Cell Reports.
About 13-30 percent of melanomas become resistant to RAF-inhibiting drugs because of a difference in how those cells produce and process the BRAF protein. The gene these patients carry is called a BRAF V600E isoform. These RAF-resistant isoform cancers produce BRAF proteins that become active complexes with another cancer-promoting protein called MEK.
Dr. Aplin, together with first author Michael Vido, an MD/PHD student in Dr. Aplin’s lab and colleagues, showed that when they blocked this complex, or dimerization, by targeting a specific site on the BRAF isoform, they could block MEK binding and restore the potency of the RAF-inhibitor.
“The work helps explain dual hypotheses for RAF-inhibitor resistance, one which focused on MEK and the other on dimerization,” said Dr. Aplin. “This work weaves the two together mechanistically. The results may also help guide the design of better combination therapies for melanoma.”
“This pivotal study is part of a much larger effort within the Sidney Kimmel Cancer Center at Jefferson to advance the pace of discoveries leading to clinical translation,” said Karen Knudsen, Ph.D., Enterprise Director of the Sidney Kimmel Cancer Center. “Dr. Aplin’s findings bring critical insight into the molecular underpinnings of therapeutic resistance, and nominate new possibilities for treating advanced disease.”
A community has rallied around a family whose car was stolen while their 11-year-old daughter was at Children’s Hospital Colorado battling cancer for a third time. KoriRae, who was first diagnosed with Leukemia in 2007, was in from Fort Collins with her mother, Jennifer Tyler, at the time of the July 13 theft.
“It was gone, I was shocked,” Tyler told CBS 4. “I couldn’t believe it.”
They had been staying at a hotel near the hospital as they are scheduled to move across the country so that KoriRae could begin new treatments at Children’s Hospital of Philadelphia. Surveillance footage captured two suspects breaking into the car and driving off. In addition to their vehicle, the thieves also made off with a stroller that KoriRae uses.
Tyler had referred to the car as the family’s lifeline, as they used it to shuttle KoriRae back and forth to crucial appointments. A GoFundMe page was started to help the family with transportation until they found a more permanent solution.
Police in Aurora located the 2000 blue Subaru Legacy a few weeks later, but the vehicle was damaged and missing all four tires, as well as KoriRae’s stroller, CBS 4 reported. That’s when police reached out to vendors in the community and asked for help.
“Obviously this is a very difficult time for this family with what they’re going through so we’re trying to do what we can to make this time just a bit easier,” Police Chief Nick Metz told CBS 4.
A local auto shop, M&M Auto Reconditioning Inc., fixed the car, while someone else donated a new stroller.
“I couldn’t believe everybody just wanted to pull together and do all this for us,” Tyler told CBS 4. “It’s something I definitely was not expecting.”
The 7-year-old girl who wished to meet Pope Francis after she was diagnosed with an inoperable brain tumor died on Monday, her family said in a Facebook post. Philomena Stendardo, of Pennsylvania, received her diagnosis in September after her father noticed her acting odd during soccer practice, Fox 29 reported.
Shortly after, her family started updating supporters with the hashtags #PrayforPhil and #StormTheHeavens, and she was contacted by the Make A Wish Foundation. Philomena asked if she could meet Pope Francis, which was made possible in November.
After announcing their daughter’s death, the family vowed that their message of prayer would not change.
“Philomena’s purpose was, and always will be, to bring people back to our Lord, WHERE WE ALL BELONG!!” a July 24 post said, in part. “Don’t you DARE turn your back on him now. Doing so would break Philomena’s heart. Saint Philomena of Port Richmond is now with the only person who loves her more than Mark and I do. The smile on her face when she went home, and the glow around her, told us all how happy she is.”
The post urged supporters to continue praying for a cure for others.