White coating on the tongue is usually not a serious disease and is easily treated, but this is not a reason to give up on the problem and postpone a visit to the dentist until better times. In this post, we look into some of the causes of this condition.
What causes white coating ?
There are many reasons. If the condition is associated with inflammation of the papillae (hypertrophy), the cause may be poor hygiene, dehydration, mechanical irritation of the soft tissues, a burn, a new diet, or excessive alcohol consumption.
If the symptoms do not go away for several days or get worse, a white coating may indicate some diseases. For example, lichen planus, which affects more than just the oral tissues, can present with white patches on the tongue, inside of the cheeks, and inflamed gums. Oral thrush is a fungal infection with vivid symptoms that causes a lot of inconvenience, but is easily treatable. Or leukoplakia – a disease of the mucous membrane. It appears as white spots that cannot be removed mechanically.
When should you see a doctor?
It is worth visiting a therapist or dentist if the tongue begins to hurt, and the pain does not go away or intensifies. Also, the reason for a visit to a specialist should be white spots on the tongue – if you find them, do not delay going to the doctor until better times.
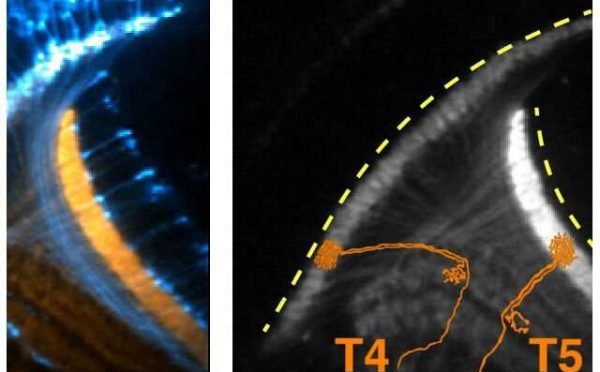
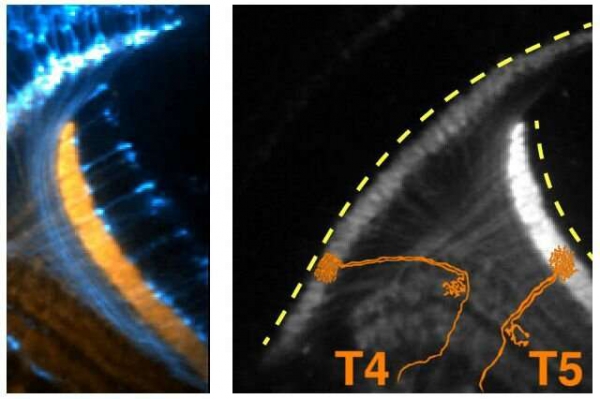
The UCLA scientists observed consistent bursts of electrical activity in the developing brain of fruit flies. T4 and T5 indicate individual neurons firing.
Neurons somehow know which of their neighbors to connect with and which to avoid in the crowded environment of the central nervous system. But how?
Using fruit flies, neuroscientists from the David Geffen School of Medicine at UCLA observed that neurons displayed periodic bursts of electrical activity early in brain development, when the larva is still developing. The coordinated activity appears to be internally driven—not triggered by something outside of the brain. The findings suggest that the signals could help neurons find each other to form networks and wire the developing brain.
The scientists imaged the electrical activity of 15 types of neurons in the brain region involved in processing vision. All of the cells fired signals at each other for two days until the adult fly emerged. Of note, the consistent firing bursts reflect patterns of connectivity that have already been recognized in the adult fly’s brain.
The authors suspect that the signaling ensures that connections established in the absence of cellular communication work properly in larger networks of neurons that collaborate to carry out specific functions.
Although this type of developmental spontaneous activity has been known for 30 years to occur in humans and other vertebrates, the UCLA study is the first time that scientists have observed it in an insect whose brain was believed to develop in the absence of such activity. The discovery of a similar phenomenon in the fruit fly suggests that neurons’ activity during development may be an essential phase of building a complex brain.
The scientists’ next step will be to explore where the activity originates, how it’s organized across the brain and how it contributes to brain development.
The findings were published online by Neuron and will appear later in the journal’s print edition.
New research from King’s College London and UCL challenges the idea that a child’s weight largely reflects the way their parents feed them. Instead, parents appear to adopt feeding styles in response to their children’s natural body weight, which is largely genetically influenced.
With childhood obesity at critical levels, researchers are looking for environmental factors which could explain why more children are developing overweight. The way a parent feeds their child is thought to be a powerful shaper of their children’s eating behaviour: rigid restriction is thought to cause weight gain because children overeat when the restriction is no longer in place (called the ‘forbidden fruit’ effect); while pressuring a child to finish everything on the plate is thought to provoke anxiety in children with low appetites and compromise weight gain.
In a study published in PLOS Genetics, the researchers looked at the relationship between a child’s genetic predisposition towards a higher or lower weight and their parent’s feeding practices. It is well established that body weight has a strong genetic basis, with up to 80% of differences between people accounted for by genetic factors.
Lead author, Saskia Selzam from the Institute of Psychiatry, Psychology & Neuroscience at King’s College London, says: “We found that parents whose children were genetically predisposed to have a lower weight were more pressuring of them to eat, and those parents whose children were genetically predisposed to have a higher weight were more restrictive over how much and what they were allowed to eat.”
“Our findings suggest that parents develop their feeding practices in response to their child’s natural tendency towards a higher or lower weight. The way a parent feeds their child may also influence their child’s weight to some extent, but our results challenge the prevailing view that parental behaviour is the major influence on childhood weight.”
The study included data from around 4,500 twin pairs who were born in England and Wales between 1994-1996 from the Twins Early Development Study, which is funded by the Medical Research Council.
By comparing twin pairs, the researchers found that many of the genes that influence individual differences in children’s weight also influence parental feeding behaviour, so that genes linked to higher weight were linked to restrictive feeding practices while genes linked to lower weight were linked to pressuring feeding practices.
Individual genetic scores were also calculated which reflected each child’s predisposition to be of a higher or lower weight based on DNA differences linked to body weight. These ‘polygenic’ scores were associated with parental feeding style and the association remained unchanged after accounting for genetic and environmental factors that are shared within a family.
Even within families where non-identical twins differed in their genetic predisposition, parents were more restrictive with the twin who had a tendency to be of a higher weight and were more pressuring of the twin who had a tendency to be of a lower weight.
Senior author, Dr. Clare Llewellyn from UCL, says: “These results show that parents are not the ‘full story’ when it comes to a child’s weight, and blaming parents for being too controlling about feeding may be unfair. But it is unclear whether these natural ‘go to’ strategies are helpful, harmful, or of no consequence to a child’s weight in the long run.”
“Large-scale randomised controlled trials which follow children from early life to later childhood are needed to test if a parent’s feeding practices can influence their child’s eating behaviour and weight.”
Breast-feeding at age 2 or older increases a child’s risk of severe dental caries by the time they’re 5, independently of how much sugar they get from foods, researchers say.
To investigate the effect of prolonged breastfeeding on children’s teeth, Karen Glazer Peres of the University of Adelaide in Australia and colleagues analyzed data on 1,129 children born in 2004 in Pelotas, Brazil, a community with a public fluoridated water supply.
Breas-tfeeding information was collected at birth and when children were 3 months, 1 year and 2 years old. Sugar consumption data was collected at ages 2, 4 and 5.
By age 5, nearly 24 percent of children had severe early childhood caries, which researchers defined as six or more decayed, missing or filled tooth surfaces, according to the report in the journal Pediatrics. Close to half of children had at least one tooth surface affected.
Children who had breast-fed for at least two years, which was close to one-quarter of the group, had a higher number of teeth that were decayed, missing or had a filling. Their risk of having severe early childhood caries was also 2.4 times higher compared with those who were only breastfed up to 1 year of age. Breast-feeding for 13 months to 23 months had no effect on dental caries.
To collect data on sugar consumption, the team used a list of food items or food groups consumed the day prior to a clinic visit. At age 2, groups were categorized as "low sugar consumption," meaning zero or less than twice daily, and "high sugar consumption," meaning two or more times daily.
But sugar consumption was only associated with a greater risk of having severe early childhood dental caries when children who consumed the highest amount were compared with children who consumed the least.
Subsequent analyses of prolonged breast-feeding, taking into account the pattern of sugar consumption throughout the child’s life course, showed that prolonged breastfeeding was an independent risk for severe caries and decayed, missing or filled teeth, the authors note.
"Breast-feeding is the unquestioned optimal source of infant nutrition. Dental care providers should encourage mothers to breastfeed and, likewise, advise them on the risk," Glazer Peres told Reuters Health by email.
"General recommendations such as drinking fluoridated water as well as cleaning a child’s teeth with fluoridated toothpaste before going to bed may help to prevent dental caries," she said. "These approaches are in line with most of the guidelines for practice and policy recommendations worldwide."
"There is no question that babies who breast-feed for a longer time than recommended by the American Academy of Pediatric Dentistry or the American Academy of Pediatrics have an increased cavity rate," noted Dr. Robert Morgan, chief of dentistry at Children’s Health in Dallas, Texas, who was not involved in the study.
"The issue is not entirely related to breast feeding. Babies who sleep with a bottle of milk or take a sippy cup of milk throughout the day or night also have an increased incidence of caries," he said by email.
"The real correlation of breast-feeding is perhaps the number of exposures to food and drink that a child has during the day and night due to the ease of access to mom," he explained.
"We know that after a baby eats or drinks there is a rise in bacteria and a rise in decay potential for approximately 20 minutes, (after which) bacterial growth and concurrent acid production decreases, as does the decay potential. Therefore, we recommend toddlers eat breakfast, lunch and dinner with perhaps a mid-morning snack and a mid-afternoon snack. If a parent brushes (the child’s teeth) after breakfast and dinner there are only three exposures to increased decay rate times," Morgan said.
"In my practice, for the mothers who would like to breast-feed for a longer period, we advise them to follow the recommended feeding schedule regardless of the feeding methods, whether breast, bottle or cup – feed and drink a non-water drink no more than five times a day and never at night – and we encourage the brushing schedule (after breakfast and dinner feeding)," he said.
A California girl died while undergoing a simple dental procedure on Monday, leaving her parents with unanswered questions in her death, her family said.
Daleyza Avila Hernandez, 3, was getting two teeth pulled and caps put on two others at the Children’s Dental Surgery Center in Stockton, east of San Francisco, her family told Fox 40.
Daleyza's mother is too shaken to leave the van. She says it hurts too much to be near where her daughter died. pic.twitter.com/JxlLK3kFWX
"My daughter was very healthy," Araceli Avila said. "All I did was I take my daughter to the dentist because they were going to fix her teeth, and about 30 minutes later they brought her back dead."
Avila and her husband, Jose Hernandez, recalled seeing the toddler "vivacious and full of life" just before the procedure. The parents said they weren’t allowed into the surgery room. But while waiting, Avila saw an ambulance pull up to the office.
This is Daleyza Avila Hernandez right before her appointment. Her parents say she was playing before her appointment. Hours later, she died. pic.twitter.com/naC2yIL0xO
"And I stood up and went outside because I was like, ‘they are coming for a kid,’ but I never thought it was for my child," Avila said.
A nurse told them their daughter’s heart stopped, possibly from underlying heart issues. Daleyza Avila Hernandez was taken to the hospital and pronounced dead.
David Thompson, the administrator of Children’s Dental Surgery Center in Stockton, told Fox 40 that Hernandez had a reaction to the anesthetics during the procedure. She was stabilized before being transported to the hospital, though Thompson said he didn’t know what caused her death. He added the girl’s parents weren’t allowed in the room due to sanitary rules.
STOCKTON — A 3-year-old girl died while undergoing a dental procedure in Stockton on Monday.… https://t.co/CeAkr6P4do
Thompson said staff members at the center were well trained and have years of experience.
"We’re committed to helping kids every single day. That’s our mission, that’s why we’re here. It’s risky. Not everyone wants to do it," he told Fox 40.
However, the Hernandez family said they still don’t understand what led to their daughter’s death.
The Dental Board of California said in a statement to Fox News:
"The Dental Board of California is aware of the tragic situation. An investigation is underway so specific details of the case cannot be shared at this time. Consumer protection is the board’s highest concern and we want to extend our deepest sympathy to the family."
Between 2000 and 2015, poison control centers in the United States received 188,468 calls about prescription opioid exposures in children and teens, a new study finds.
That translates to roughly 11,700 calls per year placed to poison control centers, researchers say.
"We knew that we were in the middle of an opioid epidemic across the country – certainly in central Ohio, where we’re located," said study author Dr. Marcel Casavant, who is chief of toxicology at Nationwide Children’s Hospital and medical director of the Central Ohio Poison Center in Columbus.
The study sheds light on how opioids – including painkillers like hydrocodone or oxycodone – impact young people, he told Reuters Health.
Casavant said data from the National Poison Data System shows that children age 5 and younger usually came in contact with opioids through "exploratory exposures" – such as when a child sees and eats a pill while crawling around on the floor.
Children ages 6 to 12 were usually the victims of medication errors, for example, when they were given the wrong dose or accidentally given a second dose.
Calls about teenagers and young adults were mostly due to intentional exposures, such as suicide attempts or drug abuse.
The researchers report in the journal Pediatrics online March 20 that opioid exposures among children and adolescents rose about 86 percent between 2000 and 2009 and then fell somewhat between 2009 and 2015.
The decline, Casavant said, might mean that doctors are being more careful in prescribing opioids, parents are getting better at keeping the medications out of reach or locked away, and there’s improved technology for deterring people from obtaining large amounts of opioids.
The downturn may also mean people are switching to street drugs like heroin, as opioids become increasingly more difficult to get, he cautioned.
Despite the downward trend, the number of opioid exposures among teens was still higher in 2015 than in 2000, Casavant said. Also, his team’s data doesn’t account for all exposures to opioids, only the ones resulting in calls to poison control.
A companion paper in Pediatrics March 20 reports a strong link between prescribed opioids and their recreational use. Teens who abused opioids were often prescribed the drugs at some point by a doctor.
Sean Esteban McCabe of the University of Michigan in Ann Arbor and colleagues analyzed nationally representative studies of high school seniors collected between 1976 and 2015. About a quarter of the students reported using opioids for medical and non-medical uses. Here too, medical and non-medical use of the drugs declined between 2013 and 2015.
Drs. David Rosen and Pamela Murray of West Virginia University in Morgantown write in an editorial that other research supports a recent decline in the use of opioids, but they caution that the decline is not true for all of the U.S.
"The epidemic of opioid use disproportionately affects some urban and more rural areas," they write.
Casavant advises that poisonous materials be kept out of sight and out of reach. Regarding opioids, he says, "We need to lock these up."
Joseph Hirsch is accused of posing as a dentist and possessing narcotics.
(Police Booking Photo)
A California man is accused of practicing dentistry without a license in an unsanitary office where he allegedly cooked meth. Joseph Hirsch, of Redwood City, is being held in San Mateo County jail on $500,000 bail after authorities received a tip about his alleged crimes, Mercy News reported.
Hirsch, 59, is accused of possessing and manufacturing controlled substances, possessing brass knuckles and possessing ammunition as a felon, the report said. Authorities said it was unclear if any patients had been harmed as a result of treatment allegedly provided by Hirsch.
Authorities arrested Hirsch after serving a search warrant at Thermo Dental and a three-month investigation involving California’s Department of Dentistry and the state’s Department of Justice, Mercury News reported. The office is allegedly surrounded by warehouse businesses and auto-repair shops.
A news release revealed authorities discovered a “crude dentist office,” with an x-ray machine and dental tools, as well as narcotics and equipment used to manufacture narcotics. A man who answered the phone at Thermos Dentistry told Mercury News he had no comment on the arrest.
A Washington family is seeking answers after their 4-year-old son died Friday during a seemingly routine dental procedure that reportedly involved a shot of anesthesia. Mykel Peterson, who was a patient at Must Love Kids dental practice in Vancouver, was on the autism spectrum and had trouble keeping his mouth open during appointments, KGW8 reported.
“He wouldn’t keep his mouth open so they can actually see what’s going on,” Thmeka Curry, Mykel’s mother, told the news outlet.
The dental practice specializes in treating children with developmental issues and uses a board-certified anesthesiologist. Mykel reportedly was given a shot of Ketamine, a common anesthesia drug, so that he would be sedated while the dentist checked to see if he needed a filling or crown, KGW8 reported.
“The dentist was telling me everything she did with his teeth, and she was going to check to see if he was awake yet,” Curry told KGW8.
Curry told KATU that the anesthesiologist said Mykel was given an extra dose to ensure he did not wake during the procedure.
“The anesthesiologist started to check his pulse and was shaking him and at this point I am still not aware anything happened to my son,” Curry, who was in the waiting room, told KOIN.
Staff members began administering CPR, and paramedics were called to the office. Mykel was transported to a nearby hospital where he was declared dead. A medical examiner is investigating to determine a cause of death, while a toxicology report will not be available for up to eight weeks, KATU reported.
“For me right now, it’s more of I just need to know what happened,” Curry told KATU. “So I can have that closure for my son. That’s it.”
A statement from Must Love Kids Pediatric Dentistry said it would be premature to comment on the specifics of the case, but that the office has performed dentistry for pediatric patients under deep sedation and general anesthesia more than 1,900 times without incident over the last three years.
“We contract with an independent, highly qualified and experienced board-certified anesthesiologist for anesthesia services who follow strict protocols, including a pre-operative checkup and clearance by the child’s primary physician prior to the procedure,” the statement said.
A GoFundMe page set up to cover costs of Mykel’s funeral said he will be remembered as a loving, energetic and smart boy.
Daisy Lynne Torres died during a dental procedure.
(GoFundMe)
The family of a Texas toddler who died during a dentist appointment has filed a wrongful death lawsuit alleging that the procedure was unnecessarily performed as part of a money-making scheme. Daisy Lynne Torres died March 29, 2016, with authorities listing anesthesia administered for the treatment of tooth decay as the cause.
Betty Squier, Daisy’s mother, said that the dentist, Dr. Michael Melanson, informed her that her child had six cavities, which was four more than initially suspected, WDTN.com reported. Dr. David Williams, a mobile anesthesiologist with Texan Anesthesiology, reportedly was present for the procedure but did not tell Squier what it entailed.
A subsequent forensic dental examiner’s report questioned why Daisy underwent the procedure, as he found no indication of dental disease or pathology in X-rays from the March 29 visit, WDTN.com reported. The $1 million lawsuit names Austin Children’s Dentistry, Melanson, Williams and Texas Anesthesiology Association, and alleges the procedure was an attempt to bill Medicaid for unnecessary dental work.
“He was committing fraud,” Squier told WDTN.com. “He was doing unnecessary work to her teeth that didn’t need to be done. He was taking advantage of a little girl. He was taking advantage of parents that didn’t know any better. We’re not doctors. We trust our medical professionals to tell us what would be the right thing to do for our children, and he completely took advantage of us.”
Every 25 minutes, a drug-addicted baby is born in the U.S.
To try to protect the youngest victims of the nation’s opioid epidemic, Tennessee enacted a law that sent new mothers to jail for substance abuse, while other states employ existing child-abuse laws to punish prenatal drug users and remove their children.
But sanctions have backfired, serving only to drive pregnant women away from necessary prenatal care and substance-use treatment, pediatricians say in three new papers.
In one, published this week in Pediatrics, the American Academy of Pediatrics exhorts policymakers to support a public health approach – rather than a criminal justice response – to opioid use in pregnancy.
"I don’t think these laws are in the best interests of moms or babies," Dr. Stephen Patrick, lead author of the report in Pediatrics, said in an interview. "Opioid-use disorder is a medical problem and not a moral failing."
Patrick is a professor at Vanderbilt University School of Medicine in Nashville, Tennessee, where he treats infants suffering withdrawal from opioids.
Instead of jail, he called for improved access to long-term contraceptives and substance-treatment programs designed to care for pregnant women.
About 100 substance-using new mothers went to jail in Tennessee between 2014 and 2016 under a fetal-assault law that’s no longer in effect, Patrick said.
The law incited so much fear in pregnant addicts that some refused to go to the hospital and gave birth at home, in cars or on the side of the road, he said.
Meanwhile, the number of pregnant women who use opioids and the number of babies born with withdrawal symptoms continues to rise.
Patrick estimated that as many as 440,000 substance-exposed infants are born in the U.S. every year and asserted: "We’re not going to arrest 440,000."
Dr. Mary Beth Sutter, a professor at the University of New Mexico in Albuquerque, works with expectant drug addicts in her state, where prosecutors charge pregnant drug users under child-abuse laws, she said in a phone interview.
"Putting women in jail and taking their babies away to try to prevent substance abuse really isn’t working," she said. "It does nothing to help these women and children, but it tends to turn them way from care."
Newborns who stay with their mothers require fewer days in the hospital, cutting the cost in half, Sutter writes in a new review in the journal Obstetrics and Gynecology Clinics of North America.
Physicians can better help drug-addicted infants when they know mothers are using illicit substances. But expectant mothers worry so much about being stigmatized, jailed and having their babies taken from them that they frequently fail to disclose drug use, Sutter writes.
Carrying a baby motivates substance users to quit. "If there ever was a time when it’s good to help people with substance abuse," Sutter said, "it’s pregnancy."
But the demand for substance-treatment programs designed to meet the unique needs of pregnant women and their babies far outstrips their availability. Only 19 states have such programs.
New Mexico has only one in-patient treatment program with just six beds for pregnant and parenting women in the entire state, Sutter said.
Medication-assisted therapy with methadone or buprenorphine has become standard care for pregnant women with opioid-use disorder, Patrick writes. But women who fear losing custody of their babies sometimes avoid treatment so as not to raise suspicion, according to another new report in the Journal of Substance Abuse Treatment.
Psychologist Dennis Hand, a professor of obstetrics and gynecology at Thomas Jefferson University in Philadelphia, examined opioid use in pregnancy throughout the U.S. and found the problem particularly acute in the South.
Southern states have fewer drug-treatment facilities, and more women take benzodiazepines, a class of sedatives and anti-anxiety drugs, along with opioids, Hand found. The combination complicates treatment for mothers and babies.
Southern women also are less likely to have health insurance, and the South has even fewer treatment programs for pregnant women than other areas, Hand said. Tennessee does not cover methadone, and Mississippi has only one methadone clinic, compared to California, which has 138, he said.
The number of infants experiencing opioid withdrawal after birth, or neonatal abstinence syndrome, grew nearly fivefold over the past decade, Patrick writes.
Many of the mothers of newborns that Patrick and Sutter treated had no idea that taking doctor-prescribed pain relievers could lead them and their babies to addiction. Sutter said her patients frequently were prescribed opioids following car accidents, dental surgeries and cesarean sections for previous births.
From 1999 to 2010, fatalities from opioid overdose have quadrupled with many of these cases involving teens, according to a JAMA study. Believe it or not, misuse of opioids often begins in the dentist’s office.
The American Dental Association recently reported dentistry is responsible for prescribing 12 percent of all instant-release opioids. Dr. Mojgam Fajiram, DDS, of Sutton Advanced Cosmetic Dentistry talked to Fox News’ Dr. Manny Alvarez about the problem.
“Our industry gives out opioids way too quickly, just to treat chronic pain,” Fajiram told Fox News, adding that, since people don’t like seeing the dentist, it’s easier for them to write an opioid prescription when a patient has pain and to say, “Don’t call me, just come see me in seven days and everything will be better.”
With dental procedures, patients don’t actually need opioids, Fajiram said. In fact, taking a combination of acetaminophen and ibuprofen will decrease the inflammation without the adverse effects of vomiting, headache and nausea— and abuse.
“There’s really no need for [narcotics] if you have a root canal, unless you’re really inflamed,” she said.
Fajiram has noticed many patients, especially younger ones, coming to the office specifically asking for the prescription painkiller they want.
“My answer to them is, ‘No.’ If you really have a lot of pain, you take Advil, you just mix it with Tylenol and you should be fine,” she said.
Other alternatives to powerful painkillers include icing the affected area for 20 minutes on and 20 minutes off to decrease inflammation, using a mouthguard or injecting Botox to control jaw joint pain, and trying acupuncture.
“Even for gum surgery, even for extraction, unless it’s impacted, you just don’t need to take any opioid,” Fajiram said.
Unfortunately, there isn’t much conversation in the dental community around the opioid epidemic, Fajiram noted. The Drug Enforcement Administration requires dentists to e-Prescribe drugs electronically, rather than by a traditional written order, which adds regulation so a patient can’t get a powerful painkiller from his oral surgeon, then go to his dentist to ask for the same drug.
“We get alerted, the pharmacy gets alerted, so that helps a little bit to regulate it,” she said.
Fajiram noted that patients who have children should be extra careful with opioid prescriptions, as the drugs are likely to get into the medicine cabinet.
When she was just 11 months old, Billie Sue Wozniak’s daughter Juno was diagnosed with type 1 diabetes, an autoimmune disease that affects 1.25 million people and approximately 200,000 children under age 20 in the United States.
The disease had affected several members of Billie Sue’s family, including her uncle, who passed away at the age of 30.
“My first thought was, ‘Her life is going to be short,’” the 38-year-old from Reno, Nevada recalled. “The more that I learned, the more I found that many people with type 1 live longer and the treatment advances are really exciting.”
While looking for treatments, Wozniak learned about encapsulation therapy, in which an encapsulated device containing insulin-producing islet cells derived from stem cells is implanted under the skin. The encapsulation device is designed to protect the cells from an autoimmune attack and may help people produce their own insulin.
After learning of the therapy through JDRF, Wozniak saw an ad on Facebook for Store-A-Tooth, a company that offers dental stem cell banking. She decided to move forward with the stem cell banking, just in case the encapsulation device became an option for Juno.
In March 2016, a dentist extracted four of Juno’s teeth, and sent them to a lab so her stem cells could be cryopreserved. Wozniak plans to bank the stem cells from Juno’s molars as well.
“It’s a risk—I don’t know for sure if it will work out,” Wozniak said.
Dental stem cells: a future of possibilities
For years, stem cells from umbilical cord blood and bone marrow have been used to treat blood and bone marrow diseases, blood cancers and metabolic and immune disorders.
Although there is the potential for dental stem cells to be used in the same way, researchers are only beginning to delve into the possibilities.
“Dental stem cells are not science fiction,” said Dr. Jade Miller, president of the American Academy of Pediatric Dentistry. “I think at some point in time, we’re going to see dental stem cells used by dentists…on a daily practice.”
Dental stem cells have the potential to produce dental tissue, bone, cartilage and muscle. They may be used to repair cavities, fix a tooth damaged from periodontal disease or bone loss, or even grow a tooth instead of using dental implants.
In fact, stem cells can be used to repair cracks in teeth and cavities, according to a recent mouse study published in the journal Scientific Reports.
There’s also some evidence that dental stem cells can produce nerve tissue, which might eliminate the need for root canals. A recent study out of Tufts University found that a collagen-based biomaterial used to deliver stem cells to the inside of damaged teeth can regenerate dental pulp-like tissues.
Dental stem cells may even be able to treat neurological disorders, spinal cord and traumatic brain injuries.
“I believe those are the kinds of applications that will be the first uses of these cells,” said Dr. Peter Verlander, Chief Scientific Officer for Store-A-Tooth.
When it comes to treating diseases like type 1 diabetes, dental stem cells also show promise. In fact, a study in the Journal of Dental Research found that dental stem cells were able to form islet-like aggregates that produce insulin.
Unlike umbilical cord blood where there’s one chance to collect stem cells, dental stem cells can be collected from several teeth. Also, gathering stem cells from bone marrow requires invasive surgery and risk, and it can be painful and costly.
The stem cells found in baby teeth, known as mesenchymal cells, are similar to those found in other parts of the body, but not identical.
“There are differences in these cells, depending on where they come from,” Verlander said.
What’s more, mesenchymal stem cells themselves differ from hematopoietic, or blood-forming stem cells. Unlike hematopoietic stem cells, mesenchymal stem cells can expand.
“From one tooth, we expect to generate hundreds of billions of cells,” Verlander said.
Yet the use of dental stem cells is not without risks. For example, there’s evidence that tumors can develop when stem cells are transplanted. There’s also a chance of an immune rejection, but this is less likely if a person uses his own stem cells, Miller said.
The process for banking stem cells from baby teeth is relatively simple. A dentist extracts the child’s teeth when one-third of the root remains and the stem cells are still viable. Once the teeth are shipped and received, the cells are extracted, grown and cryopreserved.
Store-A-Tooth’s fees include a one-time payment of $1,749 and $120 per year for storage, in addition to the dentist’s fees for extraction.
For families who are interested in banking dental stem cells, they should know that they’re not necessarily a replacement for cord blood banking or bone marrow stem cells.
“They’re not interchangeable, we think of them as complementary,” Verlander said.
Although the future is unclear for Juno—who was born in 2008—her mom is optimistic that she’ll be able to use the stem cells for herself and if not, someone else.
Ultimately, however, Wozniak hopes that if dental stem cells aren’t the answer, there will be a biological cure for type 1 diabetes.
“I hold out hope that somewhere, someone is going to crack the code,” she said.
Julie Revelant is a health journalist and a consultant who provides content marketing and copywriting services for the healthcare industry. She’s also a mom of two. Learn more about Julie at revelantwriting.com.