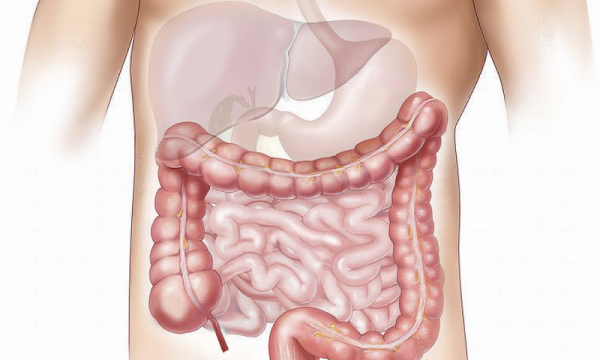
Wilson disease (copper storage disease) is a rare genetic disorder in which one or more genetic mutations disrupt copper metabolism in the liver. At some point, the liver becomes incapable of eliminating copper with bile, and copper accumulates in the liver, eyes and central nervous system. This results in serious liver damage and neurological problems inter alia. MedUni Vienna researchers led by hepatologist Peter Ferenci have now discovered that a recently described genetic mutation protects against fatty liver – apparently via vitamin A metabolism –and also ensures a better outcome for Wilson disease patients. In future, this finding could prove very useful in the personalised treatment of such patients.
The gene that has been identified is “HSD17B13,” which, according to Ferenci, plays an important role in vitamin A metabolism. Follow-up studies are planned to establish whether Wilson disease patients could benefit from this knowledge and potential treatment through the administration of vitamin A. Overall, this genetic mutation was found in every fourth person (around 26 percent). “We can assume that the HSD17B13 gene plays a critical role in the progression of Wilson disease,” explains Ferenci. “If patients do not have this mutation, their prognosis is poorer. So, in the spirit of precision medicine, we are able to predict much more accurately how the disease will progress.
In a highly regarded study published in Hepatology in 2018, the researchers showed that the protein ATP7B, known as the Wilson disease gene, and of which there are hundreds of mutations, did not provide any definitive information regarding prognosis.
Wilson disease can go undetected for years, and is usually discovered by accident. The age range is huge: The youngest known case in Vienna is a two-year-old child and the oldest patient was 74 years old. Even the symptoms are diverse: The disease can be symptomless for a long time or manifest in the form of severe liver damage, Kayser-Fleischer rings in the eyes (corneal changes) and neurological problems including movement disorders such as twitching or tremor in the limbs or even slurred speech and difficulty in swallowing. “In addition to that, there are often psychiatric disorders such as compulsive behaviours through to psychosis,” adds Ferenci.
Is your face long? Wide? Big nose? Small ears? High forehead?
It’s our faces that characterise how the world sees us, and how we recognise our close friends and family. If you’re lucky enough to be born with a highly symmetrical or a very unique face, perhaps you might have a career as a model or actor.
But how do our faces come about – and what happens when things go awry? We need to look way back to the early stages of life to find out.
From a fertilised cell
Like humans, most creatures throughout the animal kingdom have an instantly recognisable face. Such distinctive features as the trunk of an elephant, the long jaws and abundant sharp teeth of a crocodile, varied shapes and sizes of bird beaks and the unique bill of the platypus are all distinct and recognisable.
Our faces arise during the earliest stages of life. And quite incredibly, the processes that give rise to all these distinctive faces – animal and human – are exceptionally well conserved (that is, haven’t changed much over the course of evolutionary history). Amongst humans and other creatures with backbones (together known as vertebrates), the genes and biological processes that make a face are really very similar.
All animals and humans start out as a fertilised cell. Through thousands of cell divisions, the tissues that will eventually make up the skull, jaws, skin, nerve cells, muscles and blood vessels form and come together to create our face. These are the craniofacial tissues.
The face is among the earliest recognisable features that form in an embryo, with the future eye, nose, ear and tissues that will eventually form the upper and lower jaws all established by about 7-8 weeks in human gestation.
Fusion of two sides
By the sixth week of human development, the major fusion processes of the face have taken place – the two sides of the developing nose will join, both to each other and to the tissue that will become the upper lip. This first fusion (the formation of the “primary palate”) establishes the correct anatomy of the face, and serves as a structural guide for the next major fusion event – that of the secondary, or hard palate.
The hard palate originates as two separate “shelves”, one from the left side of the embryo and one from the right. These shelves elevate and grow together to form one continuous structure, ultimately separating the cavities of the nose and sinuses from that of the mouth. (You can feel this hard palate with your tongue – it’s the roof of your mouth.)
Once these fusion processes are complete (by about week 9 of gestation, still well inside the first trimester), the cells of the face still continue to dynamically move, reshape, and take on functional roles. This includes forming the structural framework of the bones, the delivery of oxygen and nutrients by the blood vessels, and controlling eye and jaw movements by the facial muscles.
The formation of the face – tissues that comprise the future nose and upper lip (red), the sides of the nose (blue) and the upper and lower jaws (green) arise by the 4th week of development (A) and have migrated and fused to form a distinctive ‘face’ by the 8th week of development (D). Credit: New insights into craniofacial morphogenesis, CC BY
Sometimes things go astray
Of course, given the incredible complexity and synchronicity required for all these cells and tissues to end up in the correct space, it is perhaps very surprising that things do not go wrong in craniofacial development more often than they do.
Problems can occur with any cell types that make up the skull, face, blood vessels, muscles, jaws and teeth.
But one of the most common craniofacial defects are palatal clefts, where the hard palate does not fuse correctly, leaving children (roughly 1 in 700 worldwide) with a large gap between their nasal passages and mouth.
Although relatively easily corrected by trained reconstructive surgeons in first-world health care systems, significant ongoing healthcare is still essential.
Services such as speech pathology and psychological counselling are often required. The children also may need medical attention to improve hearing, as problems with middle ear bones often come with other craniofacial defects.
Later surgeries to correct muscular defects do not come cheaply – assuming of course that such surgical and allied health is available to the individual in the first place. This is frequently not the case outside the first world.
Understanding why problems occur
To reduce both the severity and incidence of craniofacial defects, researchers use animal model systems – particularly mouse, chicken, frog and zebrafish embryos – to try and uncover the reasons why these defects occur.
Of all craniofacial defects, 25% are attributed (at least partially) to environmental factors such as smoking, heavy alcohol or drug use, toxic metals and maternal infection (such as salmonella or rubella) during pregnancy.
About 75% of all craniofacial defects are linked to genetic factors. As most of the genes that control craniofacial development in animals also do so in humans, using these animal models helps us better understand human palate development and how specific genes are involved.
Eventually this work may lead to new prevention and treatment strategies, for example supplementing the mother’s diet with beneficial nutrients and vitamins.
An example of such an intervention is the B-vitamin folate, used to reduce neural tube defects such as spina bifida. Mandatory folic acid fortification of food in the USA in 1999-2000 resulted in a 25-30% reduction in severe neural tube defects, clearly an exceptional outcome for newborns and their families.
Through greater understanding of the genetic processes that drive facial growth, further beneficial factors will be identified that can be safely given to pregnant mothers, and give a far better start to life to children that may otherwise be born with a craniofacial disorder.
New research reveals RNAs, which are crucial for cells to produce proteins, are also involved in protein aggregation, where proteins do not fold properly and ‘clump’ together into aggregates. If cells cannot clear these away, they become toxic and prevent cells working properly. This discovery, led by scientists at the Centre for Genomic Regulation (CRG) in Barcelona, reveals that RNAs act as a ‘scaffold’ to hold several proteins that stick to RNAs together, and that certain RNA molecules with distinct properties attract more proteins and encourage proteins to aggregate. They also investigated how an RNA called FMR1 is implicated in a neurodegenerative disease called Fragile X Tremor Syndrome, or FXTAS.
Many neurodegenerative diseases are linked to protein aggregation, including amyotrophic lateral sclerosis and Alzheimer’s disease. We know that proteins can form toxic aggregates, but until now, the contribution of nucleic acid molecules such as RNA has been up for debate.
CRG researcher and ICREA Research Professor Gian Gaetano Tartaglia and CRG Alumni Teresa Botta-Orfila, and currently at Institut d’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), wanted to understand how RNA can promote aggregation. In their research, published in the journal Cell Reports, they discovered that specific RNAs do indeed interact with many proteins within cells, and that these RNAs have distinct properties – they are structured, have a long area of untranslated genetic code called a UTR region, and often contain several repeats of genetic code (called CGG expansions) within them.
“Using theoretical tools, Fernando Cid in the group investigated how an RNA called FMR1 attracts proteins in FXTAS,” explains Gian Gaetano Tartaglia. “Together with Teresa we then worked out the proteins that bind to FMR1 using novel lab approaches and identified one of them as a protein called TRA2A. Using cells, mouse models of FXTAS and post-mortem samples from patients, we confirmed that TRA2A aggregates with FMR1 in this disease and we studied the consequences of its aggregation. Now that we know the components of some of these aggregates, we can begin to understand what is causing this disease and it may reveal new ways to treat it.”
Botta-Orfila continues: “We were surprised to find that our predicted interactions could act as biomarkers for the disease. And it was particularly exciting that we detected the TRA2A protein in the brains of people with the disease – it was one of the most important findings in my time at CRG. Lots of things suddenly made sense. The TRA2A protein that we discovered was involved in FXTAS is involved in RNA splicing, a crucial process that ensures the pieces of genetic code are in the correct order and produce the right protein. Because this protein aggregates in FXTAS, it isn’t carrying out the splicing process correctly – and as a result many RNAs are altered and cannot work properly.”
And the team’s biomarker discovery has raised more interesting questions that they’d like to answer. “Many of the genes that we found were deregulated because of protein aggregation are related to brain development, which is a key factor in disease development,” explains Gian Gaetano Tartaglia.
The team now have an arsenal of proteins to test for FXTAS, and they would like to extend their work to other complex diseases. In the longer term, they would also like to discover the function of sticky RNAs. Together, this work could improve our understanding of complex diseases where proteinaggregation is important and could ultimately reveal new ways to treat them.
Two children from Europe and one from Canada, aged four, six and 10, suffer from a previously unknown disease that causes epileptic seizures, loss of magnesium and reduced intelligence. There is currently no way to treat or alleviate their symptoms.
But researchers in an international consortium have now discovered the cause of their illness. Professor Bente Vilsen and her research group at the Department of Biomedicine at Aarhus University, Denmark, are part of the consortium, which also includes researchers from universities in Germany, England, Austria, the Netherlands and Canada. The research results have been published in the American Journal of Human Genetics.
Using a genetic analysis, the researchers have discovered that the disease is caused by a newly occurring mutation in one of the sodium-potassium pump’s four forms, known as Alpha-1. Even though the children have exactly the same three symptoms, they do not have the same genetic defect, as the amino acids in the pump protein which are genetically altered are different, explains Bente Vilsen.
“It turns out that the form of sodium-potassium pump that mutates is found in both the kidneys and the brain. The mutation leads to the kidneys, which normally absorb magnesium, instead secreting the substance in the urine; however, it is not the loss of magnesium that triggers the epileptic seizures. The convulsions occur because the sodium-potassium pump is also extremely important for the brain’s functions, meaning that giving extra magnesium supplements won’t prevent the seizures,” says Bente Vilsen.
She adds that the third frightening sign of the disease, mental retardation, should probably be attributed to a lack of oxygen to the brain during the seizures.
Jens Christian Skou received the Nobel Prize in Chemistry in 1997 for discovering these molecular pumps, which are mutated in all three children. This knowledge is important, because understanding the role of the sodium-potassium pump is the first step toward developing effective treatment methods. The research group is now working toward this goal, even though the disease is rare.
“But three cases have turned up in two different places in Europe and in Canada, and they’re not likely to be the only ones,” says Bente Vilsen. She explains that the new knowledge about the disease will probably mean that medical doctors will in future be more aware that loss of magnesium in combination with epilepsy may be caused by genetic defects in the sodium-potassium pump.
“I believe that we will find many more children with the disease, and that this is a good example of why international research cooperation is absolutely necessary—there are simply too few cases of the disease for a single country to carry out the research alone,” says Bente Vilsen.
She points out that in future, it will be possible to replace sick genes with healthy ones, and that it is therefore important to know precisely which gene is affected by a mutation. She also points out that the understanding of the disease mechanisms causing rare diseases often lead to better treatment of patients with related but far more commonly occurring diseases.
Jens Chr. Skou’s sodium-potassium pump is best known as the membrane pump that is needed for the normal functioning of nerve cells, kidney cells and most of the body’s other cells.
The pump works like a battery, separating sodium and potassium on either side of the membrane. This creates an electrical current across the cell membrane that drives many other processes such as, e.g., electric conduction along the nerve cells and the absorption of magnesium and a range of nutrients from the urine into the kidney cells, so that they are not normally lost in the urine.
Jens Christian Skou, who died in early summer at the age of 99, originally had the idea that mutations in the sodium-potassium pump would be incompatible with life. But it has since been found that serious, non-fatal diseases can originate from genetic defects in the sodium-potassium pump—exactly the case with the disease afflicting the three children.
This is due to two factors. First, there are several variants of the sodium-potassium pump in different body tissues which are able to supplement each other if one of the forms does not work. And, secondly, humans have genetic material from both parents, so even in the kidneys, which in contrast to the brain contain only one variant of the sodium-potassium pump (Alpha-1), not all of the sodium-potassium pumps will be defective, but only those derived from one of the two parents.
Therefore, in both the brain and kidneys, there will be a reduced number of functioning sodium-potassium pumps, but not a total absence of pumps—because if this was the case, the children would have died before birth, as predicted by Jens Christian Skou.
The patients were discovered by medical doctors working in clinical practice. Bente Vilsen’s group contributed their expertise in examining sick sodium-potassium pumps by inserting the diseased gene in cultured cells that originally come from monkey kidneys, making it possible to measure their pump function in the laboratory. As it turned out, the three mutations each in their own way caused the pump to be unable to transport sodium and potassium.
There is a long way to go before the research results benefit the patients, as the discovery is still basic research. However, Bente Vilsen explains that Postdoc Rikke Holm from her research group recently discovered how it was possible to use an additional mutation—a so-called ‘rescue’ mutation—to nullify the effects of the disease mutations on the pump’s binding of sodium.
“This provides an insight into the molecular mechanism that we in the research group are working to use to improve the pump’s transport activities, meaning that we can possibly one day develop a drug with a similar rescue effect. In any event, that’s our hope. The fact is that it’s basic research that generates the knowledge that forms the basis for the development of the vast majority of drugs and forms of treatment,” says Vilsen.
Machine learning—a field of artificial intelligence that uses statistical techniques to enable computer systems to ‘learn’ from data—can be used to analyse electronic health records and predict the risk of emergency hospital admissions, a new study from The George Institute for Global Health at the University of Oxford has found.
The research, published in the journal PLOS Medicine, suggests that using these techniques could help health practitioners accurately monitor the risks faced by patients and put in place measures to avoid unplanned admissions, which are a major source of healthcare spending.
“There were over 5.9 million recorded emergency hospital admissions in the UK in 2017, and a large proportion of them were avoidable,” said Fatemeh Rahimian, former data scientist at The George Institute UK, who led the research.
“We wanted to provide a tool that would enable healthcare workers to accurately monitor the risks faced by their patients, and as a result make better decisions around patient screening and proactive care that could help reduce the burden of emergency admissions.”
The study, of 4.6 million patients from 1985 to 2015, was conducted using linked electronic health records from the UK’s Clinical Practice Research Datalink. A wide range of factors was taken into account, including age, sex, ethnicity, socioeconomic status, family history, lifestyle factors, comorbidities, medication and marital status, as well as the time since first diagnosis, last use of the health system and latest laboratory tests.
Using more variables combined with information about their timing, machine learning models were found to provide a more robust prediction of the risk of emergency hospital admission than any models used previously.
“Our findings show that with large datasets which contain rich information about individuals, machine learning models outperform one of the best conventional statistical models,” Rahimian said. “We think this is because machine learning models automatically capture and ‘learn’ from interactions between the data that we were not previously aware of.”
Whether machine learning models can lead to similarly strong improvements in risk prediction in other areas of medicine requires further research.