Spoiler! Measure the pressure with a tonometer if: the numbers are above 140/90 mm Hg, then this may be it. But before you make a diagnosis, you need to know a few things about blood pressure.
Pressure is a dynamic quantity, it constantly changes depending on the needs of the body. Those. if you sit quietly, it is one (x), if you decide to run, it is another (y).
In the latter case, the pressure is likely to be higher than 140/90 mmHg. But that doesn’t mean you have hypertension. It is normal when pressure rises during physical or emotional stress – this is how the body increases blood flow to organs that work at high speeds (muscles if you run, the brain if you are stressed).
When we talk about hypertension, we mean high resting blood pressure. Because it is in peace that we are most of our lives. The vessels will cope with high pressure during physical or emotional stress, mainly because it does not last too long.
But if a person has high pressure at rest, then every day, every second, the vessels rhythmically take on an increased load from the excessive shock wave that the heart creates. No breaks, no “rest”, knock after knock. This means that there is a high probability that sooner or later somewhere (more often in the brain and in the vessels that feed the heart) the vessel can “leak out” and burst. Outcome: stroke or heart attack. Often fatal.
Therefore, one of the most important factors in the diagnosis of hypertension is correctly measured blood pressure. Because the diagnosis is based only on the numbers on the tonometer. And if there is an error, then all subsequent conclusions can be flushed down the toilet – they are incorrect. As practice shows, quite a lot of patients do not pay attention to this fact.
How to measure pressure correctly? It’s very simple.
Firstly, before the measurement, you can not smoke, drink coffee, play sports – at least 30 minutes must pass.
Secondly, before the actual measurement, you need to sit on a chair and sit quietly for 3-5 minutes.
Thirdly, you need to measure the pressure not 1, but 3 times, with an interval between measurements of at least 1 minute. It often happens that the first measurement gives high numbers, and 2-3 – normal. Focus on the 3rd dimension.
Fourth, the “white coat syndrome”: if the pressure is high at the doctor’s office, but normal at home, focus on the one at home. White coat syndrome is when the patient is subconsciously afraid of the doctor, which causes the pressure to rise, as if he was in real danger. Just show the doctor the pressure figures that you recorded at home. Remember that we are interested in REST pressure, which means that you need to measure in a calm environment.
Fifth, even if you have never suffered from hypertension, the pressure should be measured at least once a year. Because the pressure “does not hurt”, does not give any symptoms. So you can live with hypertension and not even suspect about it – and this is fraught with premature death.
Sixth, if you measure pressure on different hands, focus on the hand on which the numbers are higher.
So, hypertension is when a correctly measured resting pressure is consistently above 140/90 mmHg.
Low blood pressure or hypotension is when the blood pressure monitor shows values below 90 mmHg for systolic (first digit) and 60 mmHg for diastolic (second digit).
Hypotension can be compared to body temperature: everyone is worried when it rises. Although in fact, a sharp drop in pressure is a million times more dangerous – it literally means that a person is dying. That is, it is an acute condition that requires immediate hospitalization.
When can we witness a life-threatening drop in blood pressure? With severe bleeding, myocardial infarction, hypoglycemic coma, anaphylactic shock, severe dehydration. Most likely, such a person will be unconscious or in a fainting state, and he needs to urgently call an ambulance.
“What if my blood pressure is below 90/60 mmHg, but I feel fine?” – The most important thing here is to understand when and under what circumstances it was measured. If low pressure has always been such a plus or minus, then you are healthy, it’s just ok for you. If there were complaints (dizziness, weakness, flies before the eyes), and the pressure gauge showed a lower pressure than usual, then this may indicate some kind of disease, against which the pressure decreased. This may be due to anemia, insufficiency of the thyroid gland (hypothyroidism) or adrenal cortex (Addison’s disease), etc. So, if there are complaints + pressure has decreased – go directly to the doctor for a diagnosis.
If you are a slender young lady (as most often happens), with a subtle spiritual nature and life-long low blood pressure, then alas, you can’t raise it on purpose, there are simply no such pills. Yes, this is not necessary – everything in the body is thought out individually for your constitution, and any external influences can only spoil everything.
Of the environmental recommendations for stabilizing pressure, permanent physical activity remains (load should lead to an increase in heart rate, duration of at least 30-60 minutes daily + dumbbells or a barbell 2-3 times a week), consumption of large amounts of water + salty foods (you can allow a lot of pickled cucumbers, lovely!).
If you suffer from darkening of the eyes (orthostatic hypotension) when getting up from a chair or bed, it is recommended that you do so slowly.
If you feel weak after eating, it is recommended to eat in small portions, but often.
In general, hypotension is not an independent disease, but rather a consequence of some other pathology or condition. If you feel normal with low pressure, then you can rejoice – most likely you will live longer than any hypertensive patient.
If the pressure rises episodically, is this considered hypertension?
No. Hypertension is when your blood pressure is constantly elevated at rest.
How to take the tablets for hypertension, in the morning or in the evening?
De jure look at the packaging. De facto in 99% it does not matter, since usually drugs to control pressure last more than a day. But canonically (unless otherwise stated on the package) are taken in the morning.
Many elderly Nordic walkers (who walk with poles on a regular basis) note the normalization of pressure, linking this just the same with maintaining an active lifestyle.
It’s possible. Physical activity comes first in the non-pharmacological treatment of hypertension and other cardiovascular diseases. In any case, I would not be surprised if a person with high blood pressure began to exercise and after some time his blood pressure decreased or even returned to normal.
Is it true or a myth that in youth the working pressure is slightly lower, and at a more mature age such people suffer from hypertension?
Although there are exceptions, hypertension is still a disease of the elderly. Therefore, there is nothing surprising here that in youth, blood pressure is normal, at 40-60 years old it becomes elevated. It’s all to blame for the elasticity of blood vessels that worsens with age: they become less pliable, relax worse, which is why pressure rises.
And how do you know that hypertension has “ended”? For example, a person began to behave super-super correctly, but he also drinks pills regularly. How will he understand that a “miracle” has happened and the hypertension has receded?
Most likely, such a person will experience a decrease in pressure below the usual level, because of which he may begin to feel worse (weakness, dizziness). This will be the reason to think about the abolition of pills. But it’s better not to experiment yourself – stopping the medication can lead to a reflex jump in pressure (crisis), with all the consequences.
If a person takes drugs, but he still has pressure surges, does this mean that the therapy is chosen incorrectly?
Not always – a hypertensive crisis can happen even during therapy. In order to resist it, a hypertensive patient should always have first-aid drugs on hand, such as captopril (Capoten). They need to be taken on their own with a jump in pressure, and if they don’t help, then call an ambulance.
And if I am hypotensive and my normal pressure is 100/60, what numbers do problems start with for me?
From the same ones as everyone else: if the pressure at rest is constantly above 140/90 mm Hg. (According to other recommendations above 130/80 mm Hg)
“I think it’s sort of the first indications of a coming public health crisis for veterans,” says Ramon Hinojosa, an assistant professor in UCF’s Department of Sociology and the study’s author. “Because of the wars in Afghanistan and Iraq, we have a relatively large, new, younger generation of veterans who are going to survive for 30 or 40 years after their war experience.” Credit: University of Central Florida
After the war is over, veterans face a new threat. They are more likely to have heart disease at a younger age than nonveterans, and this could herald a new health crisis on the horizon.
These results are published in a new University of Central Florida study appearing in the Journal of the American Board of Family Medicine.
“I think it’s sort of the first indications of a coming public health crisis for veterans,” says Ramon Hinojosa, an assistant professor in UCF’s Department of Sociology and the study’s author. “Because of the wars in Afghanistan and Iraq, we have a relatively large, new, younger generation of veterans who are going to survive for 30 or 40 years after their war experience.”
The study indicates that perhaps the “healthy-soldier effect” is no longer guaranteed. The effect refers to the tendency for active-duty service members to be more physically fit and less overweight than same-age, nonmilitary individuals. It’s a phenomenon that Hinojosa explores in ongoing research.
“The outcome of the analysis suggested that not only does the healthy-soldier effect not seem as potent as it once was, in fact, what I see is veterans tend to have cardiovascular morbidity earlier than nonveterans, and they tend to have a greater number of conditions,” Hinojosa says.
The researcher said the change could be due to the nature of conflict in Iraq and Afghanistan, modern warfare, changing diets, changing approaches to leisure and exercise, higher rates of obesity in younger veterans than nonveterans at the same age, and higher rates of drinking, smoking and mental illness.
In light of these results, Hinojosa said it is important for health practitioners to look closely at cardiovascular health for younger veterans so they can address preventative approaches to ward off early onset of cardiovascular diseases.
“I think that being aware we sort of have the first rumblings of what seems to be a health crisis will help us focus our attention on health resources and providing younger veterans with access to resources that can help them ameliorate the likelihood of early onset cardiovascular disease,” Hinojosa says.
The study used data from the National Health Interview Survey, a nationally representative health survey of individuals in the United States that’s conducted by the Centers for Disease Control and Prevention’s National Center for Health Statistics.
Hinojosa looked at five particular cardiovascular conditions reported in the survey and their association with veteran status and sociodemographic status, including age.
Responses from 153,556 individuals were used, and the study looked at pooled survey data from 2012, 2013, 2014 and 2015, the most recent available data at the time.
From age 35 to about age 70, veterans reported significantly more cardiovascular conditions than nonveterans. After age 70, nonveterans reported more cardiovascular conditions than veterans.
The switch could be due to fewer veterans surviving into older age because of cardiovascular diseases, Hinojosa said.
“It’s concerning to know that the physical benefits of military service seem to be not holding as well for the younger veterans,” Hinojosa says. “This suggests the health protective benefits of military service are not what they used to be. I think that should cause us to really look at what’s going on among the veterans after they leave military service.”
Repairing heart muscle damaged by a heart attack or other cardiovascular diseases is one of the “holy grails” for cardiovascular scientists. The ability to repair heart muscle—especially by using a person’s own cells—would be a significant advance that could enhance quality of life for the millions of people who suffer from a heart attack or have a chronic heart condition.
Researchers believe that human-induced pluripotent stem cells (hiPSC) are the key to unlocking this regenerative ability. By taking a tiny bit of blood, scientists can generate an individual’s patient specific stem cells and then convert them into any cell type in the body—including cardiomyocytes, the cells that make up the heart muscle. The research, however, is in its infancy and the technique is not yet ready to be deployed for human heart disease regenerative purposes.
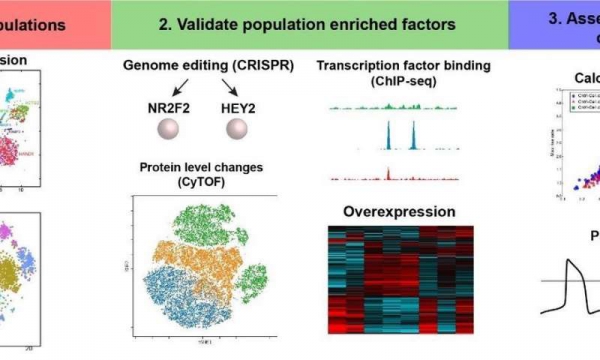
Now, researchers at the University of Arizona are one step closer to understanding hiPSC cardiomyocytes and how they may better be utilized to repair heart muscles. In a study published this month in Nature Communications, Jared Churko, Ph.D., assistant professor of Cellular and Molecular Medicine at the UA College of Medicine—Tucson, used a systems-based approach encompassing single-cell transcriptomics, single-cell proteomics and CRISPR gene-editing to identify different subpopulations of cardiomyocytes.
Definitions:
Transcriptomics is the study of the transcriptome—quantification of the types of RNA produced within the cell.
Proteomics is the study of proteomes, the proteins expressed by a cell, tissue or organism.
CRISPR gene editing is a technology for modifying an organism’s DNA code at the single-cell level. This has the potential to correct cells that are known to cause a heart condition.
The research reveals multiple subpopulations of cardiomyocytes expressing specific transcription factors (NR2F2, TBX5 and HEY2)—with different spatial and biological functions as observed in the heart. Dr. Churko believes this new understanding of cardiomyocytes can be used to better repair heart muscle injuries in the future.
“Understanding the gene signatures of different populations of hiPSC-CMs will impact our understanding of how to use such cells to discover drugs, model heart disease and repair a damaged heart,” Dr. Churko explained.
Dr. Churko’s research team included scientists from Stanford University and the Cincinnati Children’s Hospital Medical Center. Dr. Churko is associated with the Center for Innovation in Brain Science, an assistant professor of physiological sciences and genetics in the Graduate Interdisciplinary Programs, member of the Center for Applied Genetics and Genomic Medicine and the UA BIO5 Institute and director of the UA iPSC Core in the UA Sarver Heart Center.
The Nature Communications article is titled, “Defining human cardiac transcription factor hierarchies using integrated single-cell heterogeneity analysis.”
More than 8,200 women in England and Wales could have survived their heart attacks had they been given the same quality of treatment as men, according to new research.
The study did not include all hospital admissions which occurred over the 10-year study period so researchers say that the actual number of lives lost to unequal care is likely to be much higher.
Researchers from the University of Leeds used anonymised data from the UK’s national heart attack registry (MINAP) to analyse the treatment and outcomes of 691,290 people who were hospitalised for heart attack in England and Wales between 2003 and 2013.
The national registry included detailed information about each patient’s demographics, medical history and clinical characteristics such as heart rate when they entered hospital, and the investigations, treatments and procedures they received while in hospital.
In the British Heart Foundation (BHF) funded study, women tended to be older when admitted to hospital, and were more likely to have other illnesses such as diabetes and high blood pressure.
Even after adjusting for the fact that women who had a heart attack tended to be older and had more risk factors, the researchers found that women in the UK were more than twice as likely to die in the 30 days following a heart attack than men (5.2 per cent compared to 2.3 per cent). The researchers suggest that this may be, in part, explained by women being less likely to receive guideline recommended care.
Unequal care
Women who had a NSTEMI, a type of heart attack where the coronary artery is partially blocked, were 34 per cent less likely than men to receive a timely coronary angiography within 72 hours of their first symptoms (24.2 per cent of women compared to 36.7 per cent of men).
Coronary angiography creates video images to reveal narrowings or blockages in the coronary arteries. It’s a critical step in care because it helps doctors decide what to do next, and research shows that people who receive early angiography for NSTEMI have better outcomes as a result.
Women who had STEMI, a heart attack where the coronary artery is completely blocked, were 2.7 per cent less likely to receive timely reperfusion, emergency procedures including drugs and stents which help to clear blocked arteries and restore blood flow to the heart compared to men (76.8 per cent of women vs.78.9 per cent of men).
Women were 2.7 per cent less likely to be prescribed statins (87.6 per cent of women compared to 89.6 per cent of men) and 7.4 per cent less likely to be prescribed beta blockers (62.6 per cent of women compared to 67.6 per cent of men) when leaving hospital, drugs which help to lower their risk of having a second heart attack.
Although the difference in proportions may seem small in isolation, the researchers explain that even small deficits at each phase of a woman’s pathway of care can intensify into a considerable survival disadvantage.
Senior author Chris Gale, Professor of Cardiovascular Medicine at the University of Leeds and Honorary Consultant Cardiologist said: “We know women are dying due to unequal heart attack care – and now we’ve identified the shortfalls we need to target to save lives.
“For example, women not receiving coronary angiography when they arrive at hospital puts them at a disadvantage right from the start, and has knock-on effects creating further shortfalls down the line. In isolation the differences may appear small, but even in a high performing health system like the UK, small deficits in care across a population add up to reveal a much larger problem and a significant loss of life.
“We also show that not all differences are down to bias – some are down to biology. Only with more research can we hope to better understand how to target biology and best treat heart attacks in women.”
The researchers assessed the quality of care that men and women received following their heart attack based on ‘quality indicators’ – a checklist for the optimal care based on the international guidelines and endorsed by the European Society of Cardiology. Women’s care was less likely to meet 13 of the 16 heart attack quality indicators that were measured.
They estimated 8,243 deaths among women who were hospitalised with a heart attack in England and Wales could potentially have been prevented over the study period had they received care equal to that of men. But as the study did not include all heart attacks in the UK over the 10 year period, it is likely the true number of lives lost to unequal care is much higher.
The researchers point out that the differences in care likely explain much, but not all, of the gender gap in survival. Differences in heart attack symptoms, health-seeking behaviour, underlying biology, age and presence of underlying health problems, as well as response to drugs and treatments may have also played a role.
Each year in the UK around 70,000 women go to hospital due to a heart attack, and up to 25,000 women in the UK die each year from heart attacks – that’s three women every hour
Previous BHF-funded research has shown that women are 50 per cent more likely than men to receive the wrong initial diagnosis following a heart attack and are less likely to get a pre-hospital ECG, which is essential for swift diagnosis and treatment.
Professor Sir Nilesh Samani, Medical Director of the British Heart Foundation, said: “We need to tackle the false perception that heart attacks are only a male health issue. This leads to inadequate care for women – both at the time of and after heart attacks – with fatal consequences.
“While further research is needed, this study has identified several areas where heart attacks are being treated differently between the sexes, which may contribute to the worse outcomes in women. If we start to address these now, it will make a huge difference and save lives.”
(HealthDay)—There’s bad news for heart failure patients with dilated cardiomyopathy who’d like to stop taking their meds.
Any progress they’ve seen on medication is likely to fade once they stop taking their heart drugs, new clinical trial results show.
About 40 percent of a small group of patients wound up back on their medications after their heart function faltered, said lead researcher Brian Halliday. He’s a cardiovascular research fellow with Imperial College London.
“Improvement in function represents remission rather than permanent improvement for many patients,” Halliday explained.
The hearts of people with dilated cardiomyopathy can’t pump strong enough because the left ventricle of their heart has become stretched out and thin-walled.
Several different types of medications—diuretics, beta blockers, ACE inhibitors and mineralocorticoid receptor antagonists (MRAs)—can help the heart beat improve.
But these drugs can place a financial strain on patients and come with a host of side effects, Halliday said. Patients with recovered heart function often ask whether they can drop their meds.
To see whether this could be possible, Halliday and his colleagues recruited 51 heart failure patients to have their heart meds gradually withdrawn.
The patients received regular clinical reviews, followed by an evaluation at six months.
Around four out of 10 patients relapsed during the drug-withdrawal period, and had to be placed back on medication immediately.
“They did seem to recover when we put them back on medications very quickly,” Halliday said.
About half of patients completed the follow-up period without needing to go back on meds, the researchers reported.
The findings were presented Sunday at the American Heart Association annual meeting, in Chicago. Such research is considered preliminary until published in a peer-reviewed journal.
These results show that “we should tread lightly” when patients ask to be taken off their heart medications, said Dr. Jane Wilcox, an assistant professor of cardiology with Northwestern University’s Feinberg School of Medicine, in Chicago.
For the patients who relapsed, their heart failure came back “within just eight weeks of withdrawal of medication. Eight weeks. Two months,” Wilcox said.
“The question of recovery versus remission has potentially been answered by this pilot study. Currently, in 2018, we have no true signature of recovery,” Wilcox said. “These patients indeed are in cardiac remission.”
Dr. Donald Lloyd-Jones is chair of preventive medicine at Northwestern. The study helps inform “an incredibly important clinical question that comes up all the time,” he said.
“It does push us down the path of trying to understand better which patients in the future we might want to select for withdrawal of drug therapy, because no patient wants to be on more medications than they need to be,” Lloyd-Jones said. “For the time being, this class of patients is going to have to maintain their medications until we understand more.”
(HealthDay)—Another hypertension drug is being recalled due to contamination that could pose a cancer risk, the U.S. Food and Drug Administration says.
Certain lots of irbesartan are being recalled by SciGen because they contain an industrial chemical that is a suspected carcinogen, CNN reported. The recalled drugs have “Westminster Pharmaceuticals” and “GSMS Inc.” on the label.
Another heart drug, valsartan, was recalled recently due to contamination with possible cancer-causing chemicals, CNN reported.
Not all medicines that contain valsartan or irbesartan are being recalled. The new recall covers only about 1 percent of irbesartan drug products available in the United States, according to the FDA.
Amy Cavaliere and family. Two years ago, at age 35, a piece of her heart literally tore off.
Creating art and tackling do-it-yourself projects are soothing pastimes for many people, and 37-year-old Amy Cavaliere is one of them.
The mother of three from Royersford, Pennsylvania—about a half hour from Philadelphia—enjoys making pallet wall art that combines hand-stenciled words and imagery on stained wood. In fact, she was planning to franchise a popular workshop that offers classes devoted to the activity.
“You go in with friends, drink wine and make a custom piece of wooden pallet art for your home decor,” she said. “It’s fun.” Unfortunately, fate had other plans.
One morning in February 2017, while getting her children ready for school, Amy felt a heavy sensation in her chest. Her arms began to ache so badly that she couldn’t finish brushing her daughter’s hair. Within minutes, her skin turned pale and she started to hyperventilate.
Although Amy had never experienced a panic attack, that was her best guess about what was happening.
“What else could it be?” she said. After all, she was young, healthy and active, regularly participating in spinning classes and playing competitive tennis matches against her husband, John Paul.
Admittedly stubborn by nature, Amy was adamant that John Paul not dial 911. He did it anyway. Her stubborn streak continued when the paramedics arrived. She insisted upon walking to the ambulance. As paramedics checked her vital signs, she tried to convince them that she was fine.
Then her heart stopped.
As the ambulance sped to the hospital, paramedic Dave Sauls performed CPR. “I kept expecting her to come out of it,” he said, “but it wasn’t happening.”
At the emergency room, the nurses took over chest compressions and continued to perform CPR and AED shocks for nearly 45 minutes.
An angiogram revealed a 100 percent blockage of her left anterior descending artery. This type of heart attack is commonly known as the widow maker. Worse yet, the blockage was caused by spontaneous coronary artery dissection (SCAD), meaning a tear in the artery wall.
SCAD is a rare event that occurs mostly in women (about 80 percent), with an average age younger than 50. Other disorders are believed to make people more likely to suffer SCAD. One of them is a disease of the blood vessels called fibromuscular dysplasia, which Amy was later diagnosed with having.
At her local hospital, doctors decided she needed more specialized help than they could provide.
Amy spent nine days in a medically induced coma. Once she awoke, she saw John Paul sitting at the foot of her hospital bed. She had no idea of what had happened.
After the sedatives and other medications left her system, Amy felt so wired she couldn’t sleep a wink for two straight days (“my eyes were like saucers,” she said). Watching the clock tick away hour by hour, she was terrified she could experience another heart attack at any moment. Any sort of chest pain causes her anxiety to this day.
“Since I don’t remember what it felt like, I don’t have a frame of reference,” she said. “It’s terrifying—the inner turmoil of a cardiac patient.”
After 21 days in the hospital, and surviving bouts of double pneumonia and a narrowing of her trachea, Amy was released. It took more than a year for her to start feeling like herself again.
Although her heart function is permanently compromised, she is working to build strength and stamina. In the past, Amy didn’t consider it a workout unless she was drenched in sweat. But that’s no longer possible. Nor are the competitive tennis matches with John Paul.
“It’s been a hard adjustment,” Amy said. “I had to shift my mentality a bit. It’s about how much I can get done before my heart rate hits 160 bpm.”
One day, Dave Sauls, the paramedic, received a Facebook message from John Paul.
Dave had heard Amy died. So, of course, he was “flabbergasted” by the message that said she was recovering at home.
“It was a gift from God in my life and something I needed at the time,” he said. “I sat there and cried.”
Since then, Dave and Amy have become close friends. He has trained many of her friends in CPR.
Eager to raise awareness about women’s heart health in general and SCAD specifically, Amy has recorded local public service announcements and attended fundraising walks.
“I look at it as my responsibility to warn other women that this can happen to anybody,” Amy said. “I didn’t believe that it could happen to me, and my stubbornness almost cost my kids their mother.”
While it still stings that somebody else bought the home decor and art-making franchise that Amy wanted to buy into, she continues to make and sell her own pieces. She uses the name Heartwood, which her children suggested.
A Tsimane woman forages in a field. Credit: University of California – Santa Barbara
From the standpoint of heart health, the Tsimane are a model group. A population indigenous to the Bolivian Amazon, the Tsimane demonstrate next to no heart disease. They have minimal hypertension, low prevalence of obesity and and their cholesterol levels are relatively healthy. And those factors don’t seem to change with age.
Also minimal is the incidence of Type-2 diabetes. Which leads scientists to consider the role of diet in the Tsimane’s cardiovascular health—and how it might be impacted over time as the population becomes more exposed to globalization and market forces.
That’s where UC Santa Barbara anthropologists Thomas Kraft and Michael Gurven come in. They are part of the Tsimane Health and Life History Project, supported by the National Institutes of Health, which conducted the first systematic study that examines what the Tsimane consume on a regular basis and compares it to that of the Moseten, a neighboring population with similar language and ancestry, but whose eating habits and lifeways are more impacted by outside forces. The researchers’ findings appear in the American Journal of Clinical Nutrition.
“Our prior work showed that the Tsimane have the healthiest hearts ever studied, so naturally there’s a lot of interest in understanding why and how,” said Michael Gurven, a professor of anthropology at UC Santa Barbara, co-director of the Tsimane Health and Life History Project and the paper’s senior author. “The obvious first contender is, what are they eating? And are they eating what we think is best for heart health?
“We conducted a detailed analysis of the Tsimane diet and then compared it to what modern Americans typically eat, and to the diets that claim to be heart healthy,” he continued. “Maybe the Tsimane just happen to follow one of those without knowing about them.” These diets—Paleo, Okinawan and DASH, among others—are often promoted because of their proposed health benefits, and in the case of Paleo, that our bodies have evolved to benefit from particular types of food.
The connection to the Moseten is an added benefit of the study. Ethnolinguistically and genetically very similar to the Tsimane, the Moseten, an isolate in Bolivia, are much more acculturated in a number of ways than are the Tsimane. “They provide a forecast of what Tsimane health might look like 20 years from now,” Gurven said. “They represent what is happening to many indigenous populations over time. To what extent may changes in their diet increase the prevalence of heart disease and diabetes?”
Using the same measurement strategy employed by the U.S. Centers for Disease Control and Prevention’s National Health and Nutrition Examination Survey, the researchers interviewed 1,299 Tsimane and 229 Moseten multiple times about everything they had eaten or drunk in the previous 24 hours. Using published and their own nutritional estimates for all items, and a variety of methods to estimate portion size, they provided a detailed breakdown of daily food intake.
The high-calorie (2,433-2,738 kcal/day) Tsimane diet was characterized by high carbohydrate and protein intake, and low fat intake (64, 21 and 15 percent of the diet, respectively). In addition, the Tsimane don’t eat a wide variety of foods, relative to the average U.S. or Moseten diet. Almost two-thirds of their calories are derived from complex carbohydrates, particularly plantains and rice. Another 16 percent comes from over 40 species of fish, and 6 percent from wild game. Only 8 percent of the diet came from markets.
Despite the low dietary diversity, the researchers found little evidence of micronutrient deficiencies in the Tsimane’s daily intake. Calcium and a few vitamins (D, E and K) were in short supply, but the intake of potassium, magnesium and selenium—often linked to cardiovascular health—far exceeded U.S. levels. Dietary fiber intake was almost double U.S. and Moseten levels.
Over the five years of study, the researchers saw the Tsimane’s total energy and carbohydrate intake increase significantly, particularly in villages near market towns. Their consumption of food additives (lard, oil, sugar and salt) also has increased significantly. The Moseten, the researchers noted, consumed substantially more sugar and cooking oil than did the Tsimane.
The conclusion: A high-energy diet rich in complex carbohydrates is associated with low cardiovascular disease risk, at least when coupled with a physically active lifestyle (Tsimane adults average 17,000 or so steps per day, compared to Americans’ 5,100). Moving away from a diet that is high in fiber and low in fat, salt and processed sugar represents a serious health risk for transitioning populations. Evidence of nutrition transition in Bolivia parallels trends in increasing body fat and body mass index among Tsimane, suggesting the low prevalence of cardiovascular disease—as among the Tsimane—may not persist.
According to Gurven, avoiding the pitfalls of changing diets and lifestyles will be critical for groups like the Tsimane. Many other indigenous populations in South America, Africa and Southeast Asia are in similar situations. And rates of obesity, type-2 diabetes and heart disease are high among indigenous groups whose lifeways are no longer traditional—including many North American Indian and Australian aboriginal populations.
And for the Tsimane, change is not far on the horizon. “This is a key time,” said Thomas Kraft, a postdoctoral researcher in anthropology at UC Santa Barbara and the paper’s lead author. “Roads are improving in the area, as is river transport with the spread of motorized boats, so people are becoming a lot less isolated compared to the past. And it’s happening at a pretty rapid pace.”
Anecdotally, Gurven added, the Tsimane Health and Life History Project’s biomedical team is seeing more diabetic patients among the Tsimane than they have previously. That’s likely due to the increased regular intake of refined sugar and fat that occurred over the course of the study. As Kraft noted, with the Tsimane’s ability to buy large kilo bags of sugar and liters of cooking oil, the researchers calculated a 300 percent rise in consumption of those products. “They’re basically deep frying and adding lots of sugar to drinks when they can,” he said.
And consuming a lot of calories. “But they’re also physically active—not from routine exercise, but from using their bodies to acquire food from their fields and the forest,” added Gurven, “which is also an important lesson. You can’t look at what you’re eating irrespective of what you’re doing with your body. If you’re physically active, you can probably get away with more flexibility in the diet.”
Calorie count aside, the high carbohydrate content of the Tsimane diet isn’t “unprecedented,” according to Kraft. “One of the other artery-protecting diets is the Okinawan diet from Japan. It comes out at about 85 percent carbohydrate. But a common feature they share is that pretty much across the board, they’re complex carbohydrates—it’s sweet potatoes in the Okinawan diet; here it’s plantains and manioc.”
The Moseten diet has fewer total calories and less carbohydrates than the Tsimane diet, but the Moseten eat a broader range offoods, including more fruits, vegetables, dairy and legumes. The Moseten also buy more of their food, including soda, bread, dried meat and processed items. The Moseten diet could provide insight into the Tsimane diet of the future, the researchers suggest. “We’re still analyzing their health indicators, but we expect the Moseten to show more risk factors related to diabetes and heart disease,” said Gurven.
In addition to finding that the Tsimane consume more calories per day than the Moseten do, the researchers note the Tsimane are also more physically active (with much of their labor devoted to the hard work of slash and burn farming, hunting, fishing and foraging). They expend more energy activity, but may also have a higher resting energy expenditure due to higher rates of infection and persistent immune activity.
Overall, the findings suggest that no single diet protocol offers the key to health. The picture is much more complicated. “It definitely sheds light on the diversity of diets that are compatible with good cardiovascular health,” said Kraft.
Added Gurven, “We’re at a unique point in history where for many of us, our daily decisions are more about what not to eat. We have to work hard not to overeat. Throughout most of human history, it was the opposite. It was so hard to get those calories we needed to survive.”
And in terms of the Tsimane’s eagerness to incorporate sugar and other additives into their diets despite the associated health risks, “Telling folks to watch what they’re eating, don’t eat too much of this or that—that mentality is hard to convey when getting food is unpredictable and a daily grind,” Gurven continued. “Getting calories cheaply with less effort—who wouldn’t?”
The glass container is filled with a gas of cesium atoms which respond to the magnetic field from the heart. The magnetic field is detected using laser light which is transmitted through the cesium atoms. Credit: Niels Bohr Institute
Hearts ‘run’ on electrical pulses—and when doctors measure the electrical activity in a person’s heart in order to determine his or hers heart condition, they generally rely on electrocardiography (ECG):
Electrodes are placed on the patient’s chest area to record cardiac electrical activity – e.g. to determine whether the heart rhythm is so irregular that treatment is required; a type of medical examination for which ECG serves well as a diagnostic tool.
Not quite so when it comes to examining fetal cardiac electrical activity – for the obvious reason that it is impossible to place electrodes on a fetus’s chest area, which makes ECG a no-go in this context. Instead doctors will typically try to get an impression of the cardiac electrical activity by conducting an ultrasound scan; which, however, will not provide precise answers as to what is wrong should the heart e.g. be beating to fast or too slow.
In a foreseeable future these problems regarding the examination of fetal cardiac electrical activity are about to be solved – thanks to the joint effort of two groups of scientists from University of Copenhagen: from Quantum Optics (Quantop) at the Niels Bohr Institute (NBI) and from Department of Biomedical Sciences, respectively.
In a research paper—which the two groups have just published in the journal Scientific Reports—they describe an experiment which demonstrates that it is indeed possible to get a detailed read-out of fetal cardiac electrical activity. That is, if you ally yourself with a cloud of caesium atoms locked up in a hermetically closed glass cell.
“Our next challenge will be to incorporate this technique in a diagnostic sensor – and that is doable”, says assistant professor Kasper Jensen, Quantop.
Kasper Jensen and Professor Eugene Polzik, head of Quantop, have been in charge of the experiment as far as tests conducted via the locked up caesium atoms go. While Bo Hjorth Bentzen, associate professor at Department of Biomedical Sciences, has coordinated the biological part of the experiment – which includes the use of isolated guinea pig hearts.
Cloud of atoms
The locked up cloud of caesium atoms is the cornerstone of a technique tailored for observations and measurements which Eugene Polzik and his team at Quantop have refined over a number of years – and applied to a number of tasks.
Put simply, the technique allows extremely precise observations and measurements at quantum level –if laser light at certain wavelengths are transmitted through the locked up atom cloud. One project, which Quantop is currently involved in, thus aims at boosting the capacity of gravitational wave detectors through the ‘cloud of atoms-principle’.
“The locked up caesium atoms are capable of detecting very small magnetic fields. That is the reason why we also started to study this technique as a possible way of measuring fetal cardiac electrical activity – through the pregnant woman’s belly. And our experiments demonstrate that this is indeed possible – which we also conclude in our article in Scientific Reports“, says Kasper Jensen.
Guinea pig hearts
In order to conduct the experiments, the Quantop-scientists needed hearts which they could measure – and these hearts were provided by associate professor Bo Hjorth Bentzen and his team at Department of Biomedical Sciences.
They chose guinea pig hearts which are similar in size to that of a human fetus at gestational age of approximately 20 weeks – and in a number of other respects also are well suited for this kind of experiments, says Bo Hjorth Bentzen, who specializes in heart rhythm analysis:
Top: Isolated guinea pig heart in a plastic container. Bottom: The measured magnetic field from the Heart. Credit: Niels Bohr Institute
“Guinea pigs have a heart rhythm fairly close to that of a human fetus – and a number of the proteins which regulate heart functions in guinea pigs resemble the corresponding proteins in humans”.
During the experiment the scientists at Department of Biomedical Sciences euthanized a total of six guinea pigs – in accordance with protocols approved by the Danish Veterinary and Food Administration. The hearts were surgically removed from the animals, cooled down – and then transported to the Quantop-lab at NBI just a few hundred meters away.
At Quantop the hearts were gradually warmed up to body temperature – and subsequently placed in a Plexiglas chamber with a constant supply of oxygen and water in the form of a salty solution. This environment made the guinea pig hearts start beating – which they would typically do for the next three to four hours.
The equipment was placed behind a magnetic shield in order to keep all outside electromagnetic activity away – and while the heart was beating, the scientists measured the electrical activity from the organ through the Plexiglas wall.
By measuring in this fashion – at a distance of approximately one centimeter and without attaching electrodes to the heart – the Quantop-scientists mimicked a situation where fetal cardiac electrical activity is recorded via an instrument placed directly on top of the pregnant woman’s belly.
In order to show that the equipment is capable of detecting electrical signals stemming from heart problems, the team of scientist from Department of Biomedical Sciences added a chemical to the salty solution that was continuously pumped into the Plexiglas chamber. This chemical changes the electrical signal in the heart – (triggering a reaction similar to what is seen in association with long QT syndrome, a hereditary heart condition) – which the system was also fully able to detect.
Future treatment
New equipment which can conduct ECG-examinations of fetuses based on the NBI-method could have a significant impact on future treatment, says Niels Vejlstrup, MD, Ph.d, and a specialist in treatment of fetal heart problems at Department of Cardiology at Rigshospitalet in Copenhagen:
“Such equipment could make a difference in relation to e.g. AV-block – a rare condition which blocks certain electrical pulses in the heart. AV-block can develop in a fetus if the mother suffers from lupus or Sjogren’s disease – and if doctors suspect that a fetus is developing AV-block, they will start treating the mother medically in an attempt to protect the fetus. However, at present we only have one option when it comes to evaluate how severely damaged a fetus’s heart conduction system actually is – namely doing an ultrasound scan. This method is encumbered with uncertainty – which is not the case when you conduct a direct measurement of fetal cardiac electrical activity”, says Dr. Vejlstrup.
Rigshospitalet is keen on participating in clinical trials in order to develop the new method, says Niels Vejlstrup – adding that the method will be equally beneficial when it comes to diagnosing all other types of fetal heart rhythm disturbances.
At room temperature
Around the world groups of scientists are developing advanced measuring-systems – in some cases based on superconductors or on the use of rubidium, a chemical element. These methods, however, require extreme temperatures – close to absolute zero at -273.15 C, or in the vicinity of +200 C.
“In both cases the temperature bars the technique from ‘just’ being incorporated in equipment designed to detect e.g. fetal heart rhythm. Our equipment, on the other hand, operates at room temperature – which is an advantage in this context. We estimate that within three years doctors can start using our equipment to measure fetal cardiac electrical activity”, says Kasper Jensen.
The principle behind the method will also be applicable to other forms of biological registrations and examinations, he says: “E.g. measuring brain activity when looking for signs of epilepsy”.
(HealthDay)—A single point-of-care troponin concentration measured on arrival to the emergency department (ED) with 15-minute turnaround time can accurately rule out acute myocardial infarction (AMI), according to a study published online Oct. 17 in JAMA Cardiology.
John W. Pickering, Ph.D., from the University of Otago in Christchurch, New Zealand, and colleagues conducted an observational study involving adults presenting acutely from the community to the ED with symptoms suggestive of AMI. On ED arrival, troponin concentrations were measured with both a novel point-of-care assay (i-STAT TnI-Nx) and a high-sensitivity troponin I assay (hs-cTnI).
The researchers found that 16.1 percent of 354 patients experienced an AMI. Overall, 24 percent of patients presented to the ED less than three hours after onset of symptoms. There was no significant difference in the area under the receiver operating characteristic curve between the TnI-Nx assay and the hs-cTnI assay (0.975 versus 0.970). Two hundred one patients (56.7 percent) were identified as low-risk with a TnI-Nx assay result of less than 11 ng/L, with sensitivity and a negative predictive value of 100 percent; in comparison, 43.5 percent of patients were identified as low-risk by an hs-cTnI assay result of less than 3 ng/L, with sensitivity and a negative predictive value of 100 percent.
“It may be possible to safely rule out AMI within 15 minutes of blood draw in the ED for a substantial proportion of patients,” the authors write.
Several authors disclosed ties to pharmaceutical companies, including Abbott, which partially funded the study.