Researchers from the University of Jyväskylä and the Research Center for Gerontology (Finland) have published data from a study that has been ongoing since 1968. They were looking for links between the behavior of 8-year-old children and how this will affect their body weight, love of physical education, smoking and alcohol addiction in adulthood.
For example, if girls were friendly and constructive in conflict situations, then this resulted in greater physical activity at the age of 40+. And if children of both sexes were noticeably more sociable than others, played more with each other, then this predicted more active drinking by girls and smoking by boys.
If the children obeyed their elders well, then in the future this manifested itself in the form of increased self-discipline and, as a result, more active sports.
It also led to higher school success during adolescence and often higher education. And this, in turn, to the less attractiveness of alcohol and cigarettes.
As for obesity, according to the findings of scientists, children with “indicators of negative emotionality” are prone to this – that is, with neuroticism. In general, this condition in adulthood often led to bad habits. And they, in turn, lead to poor health, lower life expectancy, and so on.
What conclusion can be drawn from this? The most banal. Take care of your children, educate them, let them grow up happy, successful, healthy.
In transgender women who have had their testes removed as part of the gender-affirming process, a form of estrogen called estradiol strengthens connections between areas of the brain involved in fine motor skills, learning, emotions and sensory perception, according a study to be presented Monday at ENDO 2019, the Endocrine Society’s annual meeting in New Orleans, La. These findings reflect changes on the brain that might have implications, for instance, for treating hot flashes and other symptoms in transgender women, the researchers say.
“Once transgender women have their testes removed, their bodies have no sex hormones unless they take exogenous sex hormones (e.g., estradiol) as replacement therapy,” said researcher Tayane Muniz Fighera, Ph.D., of the Hospital de Clínicas de Porto Alegre in Porto Alegre, Brazil. Without any sex hormones, transgender women have the same symptoms, such as hot flashes, that postmenopausal women have, she said.
“The disconnection between parts of the brain involved in sensory motor processing and the thalamus may be one of the causes of these symptoms,” she said. Fighera noted this is the first study to show the effect of estrogens in the connectivity of this area of the brain in transgender women who have had their testes removed, called a gonadectomy.
“Some trans women take estradiol before surgery, but stop taking it afterwards,” she said. “Our study suggests they should continue taking estradiol not only to feminize their bodies or to avoid the symptoms related to the absence of sex hormones, but also to prevent the weakening of brain connectivity between brain regions of clinical relevance.”
“This finding is a great advance for the neuroendocrinology sciences,” said lead researcher Maiko Abel Schneider, Ph.D., of McMaster University in Hamilton, Ontario, Canada.
The study included 18 transgender women who had their testes removed when they completed surgical transition. They were invited to discontinue sex hormone therapy and then go back to taking estradiol. They underwent MRI testing 30 days after they stopped taking hormones, and again 60 days after they started taking estradiol again to compare the on/off effects of estradiol.
“We found taking estradiol strengthened the thalamus’ role as a ‘relay station’ for sensory and motor information in the brain,” they explained. Almost all sensory information that goes to the brain’s cortex first stops in the thalamus before being sent on to its destination. The thalamus is subdivided into areas that have functional specializations for dealing with particular types of information.
“Although this is a small pilot study, it suggests that sex hormones are important to keep the brain connectivity in transgender women,” Fighera said.
Medical marijuana is legal in 33 states as of November 2018. Yet the federal government still insists marijuana has no legal use and is easy to abuse. In the meantime, medical marijuana dispensaries have an increasing array of products available for pain, anxiety, sex and more.
The glass counters and their jars of products in the dispensary resemble an 18th century pharmacy. Many strains for sale have evocative and magical names like Blue Dream, Bubba Kush and Chocolope. But what does it all mean? Are there really differences in the medical qualities of the various strains? Or, are the different strains with the fanciful names all just advertising gimmicks?
I am a professor in the University of Southern California School of Pharmacy. I have lived in California a long time and remember the Haight-Ashbury Summer of Love. While in graduate school, I worked with professor Alexander Shulgin, the father of designer drugs, who taught me the chemistry of medicinal plants. Afterwards, while a professor at USC, I learned Chumash healing from a Native American Chumash healer for 14 years from 1998 until 2012. She taught me how to make medicines from Californian plants, but not marijuana, which is not native to the U.S. Currently, I am teaching a course in medical marijuana to pharmacy students.
If there is one thing about marijuana that is certain: In small doses it can boost libido in men and women, leading to more sex. But can marijuana really be used for medical conditions?
What are cannabinoids?
New research is revealing that marijuana is more than just a source of cannabinoids, chemicals that may bind to cannabinoid receptors in our brains, which are used to get high. The most well-known is tetrahydrocannabinol (THC). Marijuana is a particularly rich source of medicinal compounds that we have only begun to explore. In order to harness the full potential of the compounds in this plant, society needs to overcome misconceptions about marijuana and look at what research clearly says about the medical value.
Rafael, a Chumash who shared Californian Native American cultural knowledge with anthropologists in the 1800s. Credit: Leon de Cessac
The FDA has already made some moves in this direction by approving prescription drugs that come from marijuana including dronabinol, nabilone, nabiximols and cannabidiol. Dronabinol and nabilone are cannabinoids that are used for nausea. Nabiximols – which contain THC, the compound most responsible for marijuana’s high and cannabidiol, which does not induce a high – are used to treat multiple sclerosis. Cannabidiol, or CBD, is also used to treat some types of epilepsy.
Marijuana, originally from the Altai Mountains in Central and East Asia, contains at least 85 cannabinoids and 27 terpenes, fragrant oils that are produced by many herbs and flowers that may be active, drug-like compounds. THC is the cannabinoid everyone wants in order to get high. It is produced from THC acid – which constitutes up to 25 percent of the plant’s dry weight – by smoking or baking any part of the marijuana plant.
THC mimics a naturally occurring neurotransmitter called anandamide that works as a signaling molecule in the brain. Anandamide attaches to proteins in the brain called cannabinoid receptors, which then send signals related to pleasure, memory, thinking, perception and coordination, to name a few. THC works by hijacking these natural cannabinoid receptors, triggering a profound high.
Tetrahydrocannabivarinic acid, another cannabinoid, can constitute up to 10 percent of the dry weight. It is converted to another compound that probably contributes to a high, tetrahydrocannabivarin, when smoked or ingested in baked goods. Potent varieties like Doug’s Varin and Tangie may contain even higher concentrations.
Medical properties of marijuana
But not all cannabinoids make you high. Cannabidiol, a cannabinoid similar to THC, and its acid are also present in marijuana, especially in certain varieties. But these do not cause euphoria. The cannabidiol molecule interacts with a variety of receptors – including cannabinoid and serotonin receptors and transient receptor potential cation channels (TRP) – to reduce seizures, combat anxiety and produce other effects.
The dried bud of a Kush cannabis plant. Credit: Kerouachomsky
Myrcene is the most abundant monoterpenoid, a type or terpene, in marijuana. It can relax muscles. Other terpenes such as pinene, linalool, limonene and the sesquiterpene, beta-caryophyllene are pain relievers, especially when applied directly to the skin as a liniment. Some of these terpenes may add to the high when marijuana is smoked.
What do all these varieties do?
Many different varieties of marijuana are on the market and are alleged to treat a range of diseases. The FDA has no oversight for these claims, since the FDA does not recognize marijuana as a legal product.
Strains of marijuana are grown that produce more THC than cannadidiol or vice versa. Other varieties have abundant monoterpenoids. How do you know that the strain you choose is legitimate with probable medical benefits? Each strain should have a certificate of analysis that shows you how much of each active compound is present in the product you buy. Many states have a bureau of cannabis control that verifies these certificates of analysis. However, many certificates of analysis do not show the monoterpenoids present in the marijuana. The analysis of monoterpenoids is difficult since they evaporate from the plant material. If you are looking for a strain high in myrcene or linalool, ask for proof.
Marijuana can improve several conditions, but it can also make others worse and can have nasty side effects.
As recreational use has become more widespread, marijuana hyperemesis syndrome is becoming more of a problem in our society. Some people vomit uncontrollably after smoking marijuana regularly. It can be treated by rubbing a cream made from capsaicin, from chili peppers, on the abdomen. Capsaicin cream is available in pharmacies.
Also, high THC varieties of marijuana, such as Royal Gorilla and Fat Banana, can cause anxiety and even psychosis in some people.
For some of these conditions, studies show that eating or topically applying marijuana products rather than smoking is recommended.
Clearly, more research is needed from the scientific community to help guide the appropriate, safe use of marijuana. However, the FDA does not recognize the use of medical marijuana. This makes funding for research on marijuana difficult to find. Perhaps the cannabis industry should consider funding scientific research on marijuana. But conflicts of interest may become a concern as we have seen with drug company-sponsored studies.
South Australians don’t see heatwaves as serious events and warnings do little more than ‘trigger’ common-sense behaviours like turning on the air-conditioner, new research from the University of Adelaide shows.
The research, conducted by the University’s School of Public Health, found that South Australians do not perceive heatwaves as high risk events, an attitude compounded by TV news items, which tend to show images of people enjoying the beach during heatwaves, rather than heatwaves as potentially broadly dangerous events.
Lead author Dr. Scott Hanson-Easey says news stories that include people swimming at the beach lead the majority to believe that only vulnerable people need to take care.
“For the most part, our findings showed messaging was framed in accord with media norms and values that rendered information as infotainment,” Dr. Hanson-Easey says.
“Our data suggest that TV-news reporting is most likely contributing to heatwave risk being normalised and information being met with scepticism and irritation.”
The research, an Australian first, will help guide state emergency services and other government agencies to construct more appropriate messages as current information is not reaching the right people in the right way.
“Although age and poor health has been used as key criterions to identify vulnerability and segment target audiences, we suggest that this criterion is too blunt and may be missing households who struggle with multiple and interlaced social vulnerabilities, including poor quality housing, living in ‘hot spot’ suburbs (urban heat islands caused by lack of vegetation), low SES, and health problems,” says Dr. Hanson-Easey.
“Our findings strongly suggest that, for a majority of the public, message fatigue is not being perceived in relation to heatwave warnings and messages. Heatwave information is construed as redundant – as ‘already known’ knowledge that is not adding anything new to how individuals understand heatwaves and their adaptation options.
“Communication efforts will, if they are to remain relevant, need to adjust messaging to accord with this belief and the lived experiences of the public in a capricious social, economic and environmental climate.”
Is your face long? Wide? Big nose? Small ears? High forehead?
It’s our faces that characterise how the world sees us, and how we recognise our close friends and family. If you’re lucky enough to be born with a highly symmetrical or a very unique face, perhaps you might have a career as a model or actor.
But how do our faces come about – and what happens when things go awry? We need to look way back to the early stages of life to find out.
From a fertilised cell
Like humans, most creatures throughout the animal kingdom have an instantly recognisable face. Such distinctive features as the trunk of an elephant, the long jaws and abundant sharp teeth of a crocodile, varied shapes and sizes of bird beaks and the unique bill of the platypus are all distinct and recognisable.
Our faces arise during the earliest stages of life. And quite incredibly, the processes that give rise to all these distinctive faces – animal and human – are exceptionally well conserved (that is, haven’t changed much over the course of evolutionary history). Amongst humans and other creatures with backbones (together known as vertebrates), the genes and biological processes that make a face are really very similar.
All animals and humans start out as a fertilised cell. Through thousands of cell divisions, the tissues that will eventually make up the skull, jaws, skin, nerve cells, muscles and blood vessels form and come together to create our face. These are the craniofacial tissues.
The face is among the earliest recognisable features that form in an embryo, with the future eye, nose, ear and tissues that will eventually form the upper and lower jaws all established by about 7-8 weeks in human gestation.
Fusion of two sides
By the sixth week of human development, the major fusion processes of the face have taken place – the two sides of the developing nose will join, both to each other and to the tissue that will become the upper lip. This first fusion (the formation of the “primary palate”) establishes the correct anatomy of the face, and serves as a structural guide for the next major fusion event – that of the secondary, or hard palate.
The hard palate originates as two separate “shelves”, one from the left side of the embryo and one from the right. These shelves elevate and grow together to form one continuous structure, ultimately separating the cavities of the nose and sinuses from that of the mouth. (You can feel this hard palate with your tongue – it’s the roof of your mouth.)
Once these fusion processes are complete (by about week 9 of gestation, still well inside the first trimester), the cells of the face still continue to dynamically move, reshape, and take on functional roles. This includes forming the structural framework of the bones, the delivery of oxygen and nutrients by the blood vessels, and controlling eye and jaw movements by the facial muscles.
The formation of the face – tissues that comprise the future nose and upper lip (red), the sides of the nose (blue) and the upper and lower jaws (green) arise by the 4th week of development (A) and have migrated and fused to form a distinctive ‘face’ by the 8th week of development (D). Credit: New insights into craniofacial morphogenesis, CC BY
Sometimes things go astray
Of course, given the incredible complexity and synchronicity required for all these cells and tissues to end up in the correct space, it is perhaps very surprising that things do not go wrong in craniofacial development more often than they do.
Problems can occur with any cell types that make up the skull, face, blood vessels, muscles, jaws and teeth.
But one of the most common craniofacial defects are palatal clefts, where the hard palate does not fuse correctly, leaving children (roughly 1 in 700 worldwide) with a large gap between their nasal passages and mouth.
Although relatively easily corrected by trained reconstructive surgeons in first-world health care systems, significant ongoing healthcare is still essential.
Services such as speech pathology and psychological counselling are often required. The children also may need medical attention to improve hearing, as problems with middle ear bones often come with other craniofacial defects.
Later surgeries to correct muscular defects do not come cheaply – assuming of course that such surgical and allied health is available to the individual in the first place. This is frequently not the case outside the first world.
Understanding why problems occur
To reduce both the severity and incidence of craniofacial defects, researchers use animal model systems – particularly mouse, chicken, frog and zebrafish embryos – to try and uncover the reasons why these defects occur.
Of all craniofacial defects, 25% are attributed (at least partially) to environmental factors such as smoking, heavy alcohol or drug use, toxic metals and maternal infection (such as salmonella or rubella) during pregnancy.
About 75% of all craniofacial defects are linked to genetic factors. As most of the genes that control craniofacial development in animals also do so in humans, using these animal models helps us better understand human palate development and how specific genes are involved.
Eventually this work may lead to new prevention and treatment strategies, for example supplementing the mother’s diet with beneficial nutrients and vitamins.
An example of such an intervention is the B-vitamin folate, used to reduce neural tube defects such as spina bifida. Mandatory folic acid fortification of food in the USA in 1999-2000 resulted in a 25-30% reduction in severe neural tube defects, clearly an exceptional outcome for newborns and their families.
Through greater understanding of the genetic processes that drive facial growth, further beneficial factors will be identified that can be safely given to pregnant mothers, and give a far better start to life to children that may otherwise be born with a craniofacial disorder.
Some of the damaging cell effects linked to ageing could be prevented by manipulating tiny parts of cells, a study shows.
Scientists have shed light on how the harm caused by senescence – a vital cell process that plays a key role in diseases of ageing – could be controlled or even stopped.
Researchers say the findings could have relevance for age-related diseases including cancers and diabetes, although they caution that further research is needed.
During senescence, cells stop dividing. This can be beneficial in assisting wound-healing and preventing excessive growth.
Some aspects of senescence are also harmful and can lead to tissue damage and the deterioration of cell health as seen in diseases of older age.
Scientists at the Medical Research Council’s Human Genetics Unit and the Cancer Research UK Edinburgh Centre at the University of Edinburgh focused on a chain of harmful processes triggered by senescence, known as the senescence-associated secretory phenotype (SASP).
The SASP is a cascade of chemical signals that can promote damage to cells through inflammation.
The researchers showed that manipulating a cell’s nuclear pores– gateways through which molecules enter the heart of the cell – prevented triggering of the SASP.
Findings also show that DNA had to be reorganised in space within in the cell’s nucleus in order for the SASP to be triggered.
Researchers say the study sheds light on the fundamental workings of the cell and could be instrumental in understanding cell ageing.
The study is published in Genes and Development.
Professor Wendy Bickmore, Director of the Human Genetics Unit at the University of Edinburgh’s Medical Research Council Institute of Genetics and Molecular Medicine, who led the study, said: “These findings provide us with a much clearer understanding of how senescence causes cell damage. Whilst we are some way from being able to halt the damage caused by the ageing process, we hope that this advance will open up avenues to explore how we might slow some of the harm that stems from senescence. This could be of relevance to the many conditions that tend to affect us as we grow older.”
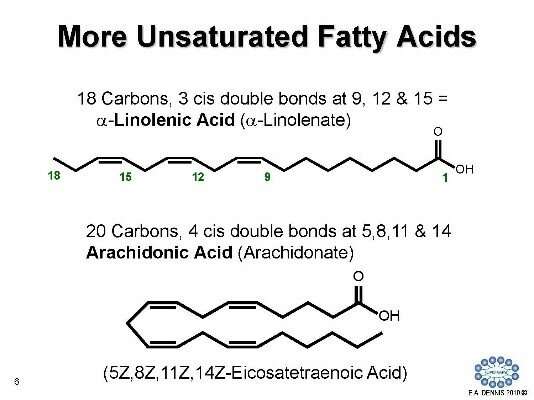
Another example of LIPID MAPS database content. Credit: Edward Dennis, UC San Diego
The post-holiday New Year might not seem like an ideal time to celebrate fat. But when it comes to lipids, there is no better time. For the past 15 years, scientists have been working to specify and classify these fatty acids in order to develop techniques, tools and terms to better study them. Now a new generation of chemists and biochemists is pounding out research to further understand the complex nature of lipids. The pending results, according to a new article in Science Signaling, could reshape the diagnosis and treatment of various acute and chronic conditions—from diabetes and atherosclerosis to cancer and auto-immunity.
Dubbed “lipidomics,” the study of lipids is weighty in terms of its potential for precision medicine—an emerging approach for treating and preventing disease by considering an individual’s genes, environment and lifestyle, according to the U.S. National Library of Medicine. With new methods for precision medicine expected to develop over the next five to 10 years, lipids are considered “phat” (i.e., excellent) candidates for integration with these emerging methodologies. This is why next-generation researchers look at lipids with a more holistic, systems biology perspective.
Biologically versatile and essential, lipids help keep cells intact, store energy and communicate signals within the body. They also function as termini for complex cellular and organ functions and denote normal and disease states. Additionally, they are easily accessible through blood and urine, and they are quantifiable. Yet advances are needed for new analytical, statistical and informatics tools to progressively study them. Since new lipids continue to be discovered, new technology is needed to reveal exactly how many lipids our cells contain, to locate new lipids and to determine in which cellular membranes lipid changes occur.
A leader on the journey of lipids research is UC San Diego Distinguished Professor and Chair of the Department of Chemistry and Biochemistry Edward Dennis. Along with UC San Diego colleagues Christian Glass, Michael van Nieuwenhze, Shankar Subramaniam and Joseph Witztum, as well as researchers from other universities, Dennis collaboratively established the gold standard classification system called LIPID MAPS in 2003, with $73 million from the National Institutes of Health (NIH). The database of about 40,000 lipid structures is referenced by the world’s lipid researchers and cited in scientific journals.
Example of information found on the LIPID MAPS database. Credit: Edward Dennis, UC San Diego
“While the LIPID MAPS Consortium included a dozen U.S. investigators sponsored by the U.S. NIH, we invited scientists from Asia and Europe to join us in developing the LIPID MAPS Classification, Nomenclature and Structural Drawing Standards that contributed to international acceptance of LIPID MAPS,” explained Dennis. “This led to the rapid development of the lipidomics field.”
Beyond its emphasis on classification and structural representation, as well as its practice of openness and collaboration, LIPID MAPS has become a significant resource that helped to usher in the bioinformatics era. Now new researchers envision a big data picture of lipids study. With recent funding from the Wellcome Trust led by Valerie O’Donnell and Michael Wakelam from Cardiff University and Babraham Institute in the UK, further development of the LIPID MAPS database and website will continue.
Michael Wakelam, Director of the Babraham Institute, which now hosts the LIPID MAPS database, said: “The new Wellcome Trust funding for LIPID MAPS is vital in allowing us to build upon the excellence of the initial system supported by NIH. We look forward to expanding the research opportunities that LIPID MAPS enables, particularly in the area of lipid pathway analysis while continuing to develop and maintain existing provisions and accessibility.”
“Lipidomics is a significant part of the metabolomics, which is a measure of all metabolites in any species. Metabolomics can differentiate between a state of wellness and illness in humans,” said Subramaniam, distinguished professor of bioengineering, who is also affiliated with cellular and molecular medicine and computer science and engineering at UC San Diego, and who serves as the Principal Investigator on the National Metabolomics Repository Grant from the NIH.
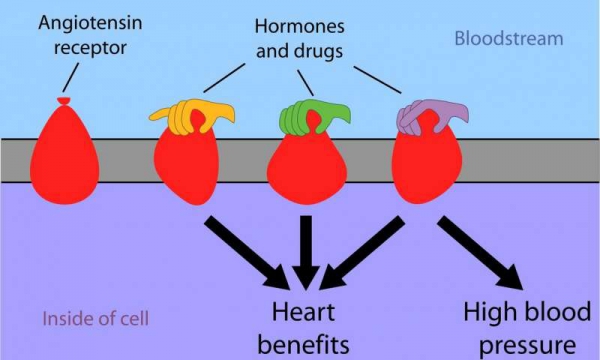
Just as squeezing the top of a balloon changes its overall shape, the interaction of hormones and drugs in the bloodstream changes the shape of cell surface receptors. A pair of new papers map those shapes in detail, giving researchers hope of developing more specific, more effective medications. Credit: Lefkowitz Lab, Duke University
Blood pressure drugs, like many medications in use today, often have ‘off-target’ effects because we don’t yet understand exactly how they work.
New research out of Duke, UCLA, Stanford and Harvard is showing precisely how the crucial cell surface receptors interact differently with various drugs, giving the researchers hope that they may be able to tailor more specific medications for heart patients.
High blood pressure affects one in three American adults, increasing the risk of heart disease and stroke for about 75 million Americans.
The blood vessel constriction which raises blood pressure is triggered by the interaction of a hormone, angiotensin II, with the angiotensin receptor on the surface of cells in the heart, blood vessels, kidney, adrenal cortex, lungs and brain. Blood pressure drugs called angiotensin receptor blockers (ARBs) treat high blood pressure by preventing angiotensin II from binding to its receptor.
But in doing so, these drugs also block angiotensin II’s beneficial effects, including increases in the heart’s strength and performance.
Ideally, physicians would like to block the angiotensin receptor’s effects on blood pressure without losing its positive effects on heart function, said cardiologist Robert Lefkowitz, M.D., the James B. Duke professor of Medicine and senior author of one of two companion papers coming out in Cell on Jan. 10.
Duke researchers collaborated with scientists across the country to determine the various shapes the angiotensin receptor assumes when it is turned on by different types of drugs, a key step towards being able to design better heart medicines.
“For a long time, people assumed that these receptors had one ‘off state’ and one ‘on state,’ like a light switch,” said lead author Laura Wingler, Ph.D., a postdoctoral researcher in the Lefkowitz laboratory. “But they aren’t light switches; these receptors are more like dials with multiple settings, or states. What’s been unclear for the past 10 years is what these receptor states look like and why each state triggers different events inside the cell.”
Just as squeezing only the top of a balloon alters its entire shape, the binding of hormones and drugs to the outside of a receptor causes changes in parts of the receptor which face into the cell. Different hormones and drugs push different “buttons” on a receptor, changing its shape in different ways.
Seeing those specific shapes of the angiotensin receptor for the first time “helps us approach the design of drugs more rationally,” Wingler said. “Now we know what to be aiming for and the mechanisms we need to target.”
The Duke-led study, which included colleagues at UCLA and Stanford, used a sophisticated technique called double electron-electron resonance spectroscopy to map the shape of the receptor when it interacts with different classes of hormones and drugs.
“It’s like seeing a silhouette of the receptor—an outline of its shape from one viewpoint,” Wingler said.
The researchers discovered that the receptor assumes four main shapes: one associated with ARBs that turn the receptor completely off, one associated with angiotensin II and drugs that turn the receptor fully on (both increasing blood pressure and improving heart function), and two associated with the drugs that improve heart function without increasing blood pressure.
In a second paper, the Duke group worked with the laboratory of Andrew C. Kruse, a professor at Harvard Medical School, to use X-ray crystallography to see the fine details of the receptor when it is frozen in the “fully on” state.
Wingler compares this approach to seeing an intricate, three-dimensional statue of the receptor. Importantly, it let them see how one drug interacts with the receptor and what “buttons” it presses to change the shape of the receptor.
The angiotensin receptor is a member of a family of proteins called G protein-coupled receptors (GPCRs), which sit in the membrane that surrounds cells and interact with hormones and drugs in the bloodstream. The GPCR family includes receptors for adrenaline, histamine, opioids, and the many molecules responsible for taste and smell, and they are the target of about one-third of all FDA-approved drugs.
Lefkowitz and Stanford University Professor Brian Kobilka, a senior co-author on one of the Cell papers, shared the 2012 Nobel Prize in Chemistry for discovering the GPCR family and defining how these receptors work.
The researchers hope these latest findings may lead to tailor-made drugs for other GPCRs that could separate desired therapeutic effects from unwanted side effects.
For example, these same principles have already been used to develop new drugs for the opioid receptor that have advanced to clinical trials. These next-generation opioid receptor drugs relieve pain but are less prone to cause the side effects associated with morphine and fentanyl, such as constipation and potentially lethal slowed breathing.
“Our papers go way beyond anything which has been done in this field before,” Lefkowitz said. “This research is likely to lead to discovery and development of novel types of drugs which can manipulate these receptors‘ shapes in ways that have not previously been possible.”
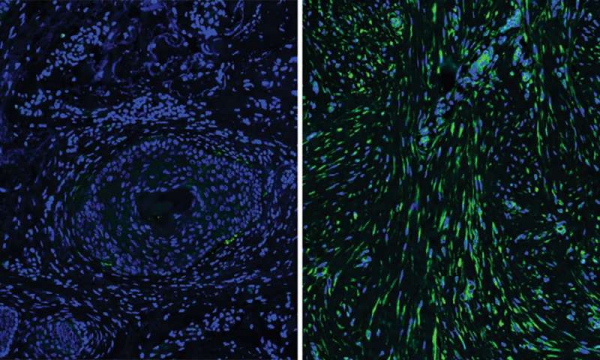
A microscopic comparison between normal skin (left) and scarred skin. Credit: Yale University
Differences in the cells that give skin its resilience and strength during wound repair may explain why individuals heal differently, according to a new Yale study published Nov. 23 in the journal Science.
Fibroblasts, the cells that form the protein structure beneath the surface of the skin, were once thought to be fairly uniform in their function. However, the new study found that subsets of fibroblasts may explain why skin regeneration is less robust in older people and how certain types of scars form.
“These subsets of cells may explain different healing potentials in different people,” said senior author Valerie Horsley, associate professor of molecular, cellular, and developmental biology.
Horsley and first author Brett Shook studied the genetics of fibroblasts and looked at their effects in mice and humans and found multiple differences in how these cells respond to injury and changes that occur during aging. For instance, after injury, a subset of fibroblasts that normally produce adipocytes, or fat cells, start forming scar tissue to repair the skin tissue. Interestingly, say the researchers, these cells are reduced in human skin compared to mouse skin, which may explain why scars are more prevalent in people than mice.
The study also identified the essential role of immune cells called macrophages in not only fighting infection but also healing wounds and scar formation. Macrophages that appear at the peak of tissue regeneration can selectively signal to a subset of fibroblasts. Human scar tissue contains more macrophages and fibroblast subsets and both populations are reduced in poorly healing wounds from aged mice.
“By identifying functionally distinct populations of skin cells and revealing the signals that control their behavior, we hope to develop new targeted therapies for the treatment of defective wound healing and scar formation,” Shook said.
Now that our days are getting colder and shorter, a new study from the University of Pittsburgh gives us reason to think about the odd relationship between alcohol and weather.
It found that throughout the world and in the United States, drinking levels and liver disease correlated with climate and sunlight. Drinking and disease rose as average temperatures and hours of sunlight fell.
The study, which was published in the journal Hepatology, has public health implications at a time when deaths from cirrhosis of the liver have been rising, particularly among 25- to 34-year-olds. Ramon Bataller, senior author and chief of hepatology at University of Pittsburgh Medical Center, said knowing that heavy drinking is more common in colder climes could help officials who want to reduce damage from alcohol to direct resources toward regions at the highest risk. He also suggested that someone with a family history of alcoholism who has a choice between jobs in, say, Missouri and Minnesota would do well to pick the warmer state.
The World Health Organization estimates that almost 6 percent of deaths throughout the world can be attributed to alcohol misuse.
Bataller said people in colder climates may drink more because alcohol tends to make them feel warmer. On the other hand, people in hot places are more likely to feel uncomfortable or light-headed when they drink. For many people, darkness can also exacerbate depression, which is associated with drinking, though alcohol is a depressant. Snowy climates might also increase isolation, which can make depression worse.
While people in frigid places like Russia are known for heavy drinking, Bataller said the connection between drinking and climate had not been studied systematically before. A team led by Meritxell Ventura-Cots, a postdoctoral researcher at the Pittsburgh Liver Research Center, used large public data sets to compare average temperature and sunlight hours with average alcohol consumption per person, binge drinking, and the percentage of drinkers in a population. They also looked at cirrhosis caused by heavy drinking. The patterns they found held up even when the team controlled for religious restrictions on alcohol use. Florida and Hawaii were exceptions, possibly because so many partying tourists visit, Ventura-Cots said.
She said the study found that in Europe, people in Ukraine drank 13.9 liters of alcohol per capita per year while warmer Italians drank 6.7 liters per capita. (A liter is about 34 ounces.) In the U.S., people in Montana drank 11.7 liters of alcohol per capita per year while people in North Carolina drank just 7.8. (That’s still more than 2 gallons.)
The researchers did not have data on whether people drink more in winter than summer.
Generally, public health officials say women should average no more than one drink per day and men no more than two. Adding another drink a day increases the risk for cirrhosis, Bataller said. Obesity and smoking further add to the risk.
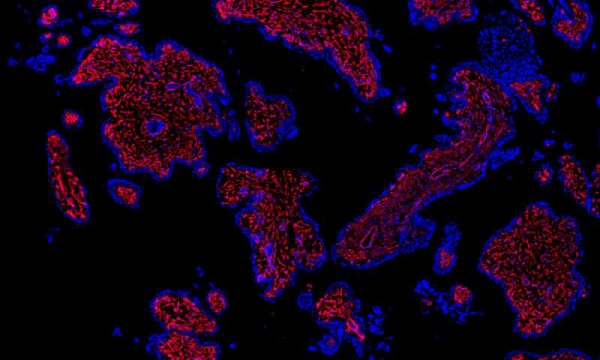
Researchers have mapped more than 20 different cell types present in the first-trimester human placenta, including stromal and endothelial cells (red). Credit: Rockefeller University
To treat and prevent pregnancy-related disorders, researchers must understand not only what can go wrong, but when. Complications, such as preeclampsia and pre-term birth, often occur in the second or third trimester, and most research to date has focused on those later stages of pregnancy. But the biological events that lead to these problems could start much earlier.
In a new Rockefeller study, published in Science Advances, scientists present the first detailed descriptions of both fetal and maternal cells that are present during the first trimester, a body of work they say could inform further research into a variety of pregnancy complications.
Parent and child, cells and genes
The researchers analyzed cells from placental and decidual, or endometrial, tissues, which allowed them to look at cellular features in the fetus and mother, respectively. In their samples they identified 20 distinct cell types—nine from the placenta and eleven from the decidua.
“It’s the first cellular atlas of the early human placenta,” says Hemant Suryawanshi, first author on the paper and a postdoctoral associate in the lab of Thomas Tuschl.
In addition to identifying different cell types, the scientists used a novel method to determine which genes were expressed by each of those cells. Previous research on first trimester tissue, explains Suryawanshi, relied on a method called bulk RNA sequencing, which generates averaged RNA profile from multiple cells, rather than specific data derived from single cells.
For this study, by contrast, Suryawanshi and colleagues used a microfluidics based single-cell RNA sequencing method to analyze more than 14,000 individual placental cells and nearly 7,000 individual decidual cells, all from first trimester tissue. No previous single-cell RNA study had looked at more than two dozens decidual cells, Suryawanshi says, and those cells were from second and third trimester tissue.
“We now have a profile for the many thousands of genes expressed by each of the 20 cell types,” he says.
Solving maternity mysteries
The atlas, says Suryawanshi, could become a useful tool for future researchers. For example, a scientist interested in first-trimester endometrial epithelial cells, which are found in the decidua and play a crucial role during embryonic implantation, could use it to see which genes those cells express, as well as the “strength of expression” of each gene, data which the new paper includes.
The need for such a tool is clear, says Zev Williams, chief of Reproductive Endocrinology and Infertility at Columbia University Medical Center, who contributed to the study. “The placenta is a profoundly important yet poorly understood organ. It is essential for life and, for our time in the uterus, functions as the lungs, kidney, liver and immune system. Yet, its structure and function are still very much a mystery.”
Part of that mystery involves the interaction between the fetus and mother during the first trimester. “Why doesn’t the mother’s immune system, as it normally would, reject the fetus, which in many ways is analogous to an organ transplant or a parasite invasion?” asks Suryawanshi.
The answer may lie in the cellular communication between the placenta and the decidua wall, which sheds off when there is no implantation.
“In the presence of pregnancy, there are dramatic changes in cellular composition and at the molecular level. Now, for the first time, we have high-resolution pictures of those changes,” he says.
And, because the atlas is a blueprint of normal first-trimester tissue and cell types, it could potentially serve as a template to help identify abnormalities at the cellular and genetic level in problem pregnancies.
“We can now begin to understand how the placenta and decidua work in concert to enable healthy pregnancies to occur,” says Williams. “By understanding, in detail, the diversity and specialized functions of cells that comprise the early placenta and the decidua, we can start to discover the underlying causes of many diseases of pregnancy and, ultimately, develop ways to improve pregnancy outcomes.”
Machine learning—a field of artificial intelligence that uses statistical techniques to enable computer systems to ‘learn’ from data—can be used to analyse electronic health records and predict the risk of emergency hospital admissions, a new study from The George Institute for Global Health at the University of Oxford has found.
The research, published in the journal PLOS Medicine, suggests that using these techniques could help health practitioners accurately monitor the risks faced by patients and put in place measures to avoid unplanned admissions, which are a major source of healthcare spending.
“There were over 5.9 million recorded emergency hospital admissions in the UK in 2017, and a large proportion of them were avoidable,” said Fatemeh Rahimian, former data scientist at The George Institute UK, who led the research.
“We wanted to provide a tool that would enable healthcare workers to accurately monitor the risks faced by their patients, and as a result make better decisions around patient screening and proactive care that could help reduce the burden of emergency admissions.”
The study, of 4.6 million patients from 1985 to 2015, was conducted using linked electronic health records from the UK’s Clinical Practice Research Datalink. A wide range of factors was taken into account, including age, sex, ethnicity, socioeconomic status, family history, lifestyle factors, comorbidities, medication and marital status, as well as the time since first diagnosis, last use of the health system and latest laboratory tests.
Using more variables combined with information about their timing, machine learning models were found to provide a more robust prediction of the risk of emergency hospital admission than any models used previously.
“Our findings show that with large datasets which contain rich information about individuals, machine learning models outperform one of the best conventional statistical models,” Rahimian said. “We think this is because machine learning models automatically capture and ‘learn’ from interactions between the data that we were not previously aware of.”
Whether machine learning models can lead to similarly strong improvements in risk prediction in other areas of medicine requires further research.
































{kind=link}
{kind=link}