Dr. Michael Rieder, professor at Western University and scientist at Robarts Research Institute with his new rapid test kit for E. coli. Credit: University of Western Ontario
A new E.coli rapid testing kit developed by researchers at Western University is revolutionizing food safety testing by producing results within hours, not days – and ensuring contaminated food doesn’t make it to the produce aisle of your neighbourhood grocery store.
The kit detects E. coli 0157, the same food-borne bacteria causing the current outbreak in the US and Canada linked to romaine lettuce. The kit has been approved by Health Canada and translated for commercial use. The first production lot of this assay was last summer and this kit is now making its way to food processing plants in North America.
“Our goal is to get the testing to occur as close as possible to the source,” said Dr. Michael Rieder, professor at Western’s Schulich School of Medicine & Dentistry and scientist at Robarts Research Institute. “This technology is not only faster, but it’s less expensive, it’s easy to use, and it can occur right in the processing plant.”
Current food testing methods typically rely on culture, which requires samples to be sent away for testing, with results taking up to two weeks to come back. By that time, the food has often been shipped to market and large recalls have to occur.
The Western-developed kit detects a protein unique to the pathogenic E. coli bacteria, and using flow through technology is able show results in hours rather than days. The process works in much the same way as a pregnancy test – showing one line for negative and two lines for positive.
“We are looking at this specific biomarker because it is unique to this pathogenic bacteria. The presence of bacteria itself isn’t bad, but we want to be able to identify specific bacteria that will cause people to get sick,” Rieder said. “The goal is a safer food chain for everyone so that public safety can be assured.”
The system was developed as a result of collaborations between Dr. Rieder, a team at International Point of Care (IPOC), and London entrepreneurs, Craig Combe and the late Michael Brock. The commercialization and sale of the kits has been accomplished with industrial partners both in Canada and the United States. Much of the work was funded through grant from Mitacs, a federal non-profit that encourages academic and industrial collaboration.
Health officials say they’ve identified two new cases of children infected with adenovirus at a New Jersey pediatric health care facility.
The Voorhees Pediatric Facility near Philadelphia tells WPVI-TV Friday that brings the total number of infected patients to 12. Facility officials say there have been no related deaths and none of the patients are in critical condition.
At least 10 people died earlier this year after an outbreak of a different strain of adenovirus at Wanaque Center for Nursing and Rehabilitation in New Jersey in Haskell, about 100 miles(161 kilometers) away. There have been 28 cases associated with the respiratory virus at the center, where the affected children had severely compromised immune systems. One death was a young adult.
Officials have said there is no wider public health concern.
University students who are Lesbian, Gay and Bisexual (LGB) are at higher risk of self-harm and attempting suicide than their heterosexual counterparts, finds new research.
The study also shows that low self-esteem may explain the increased risk of self-harm in LGB students. Low self-esteem may result in LGB students who have faced discrimination or have struggled to accept or share their sexuality with others.
The study was carried out by a team at The University of Manchester, Leeds Beckett University, Lancaster University and Edith Cowan University in Australia, and is published in Archives of Suicide Research today.
Of the LGB students who completed an online questionnaire, 65% had carried out non suicidal self-harm over their lifetime compared to 41% of heterosexual students.
Self-harm typically includes behaviour such as cutting, hair pulling, scratching, burning or non-lethal overdoses.
And 35% of LGB students had attempted suicide in their lifetime compared to 14% of non-LGB students.
The study was completed by of 707 students with an average age of 23 from two English Universities of which 119 self-identified as LGB.
The study does not tell us, however, whether being at University increased the risk of self-harm in LGB people.
And it is not possible to compare the student sample with prevalence rates for non-suicidal self-injury and suicide attempts across the population as a whole.
Dr. Taylor said: “Surprisingly, there is little data on the psychological mechanisms that might explain the association between being lesbian, gay or bisexual, and self-harm in UK students. This data highlights how low self-esteem may leave some LGB students more at risk.
“Interestingly, anxiety and depressive symptoms did not appear to be important once self-esteem was taken into account.
He added: “So prevention and intervention efforts directed at these psychological mediators by Universities may help to reduce risks in this population.
“Universities are already doing a lot of good things in this area such as counselling and psychological support which is targeted at LGB people.
“And tackling discrimination and improving acceptance of LGB people through public policy and media campaigns may be helpful in reducing any impact on self-esteem.”
Dr. Elizabeth McDermott of Lancaster University said: “Young people’s mental health is a national concern and this study confirms that lesbian, gay or bisexual young people have elevated rates of suicidality and self-harm compared with heterosexual youth. We know much less about how LGB young people seek help for their mental health problems, or what type of support would be effective.”
The paper Psychological correlates of self-harm within gay, lesbian and bisexual UK University students, is published in Archives of Suicide Research.
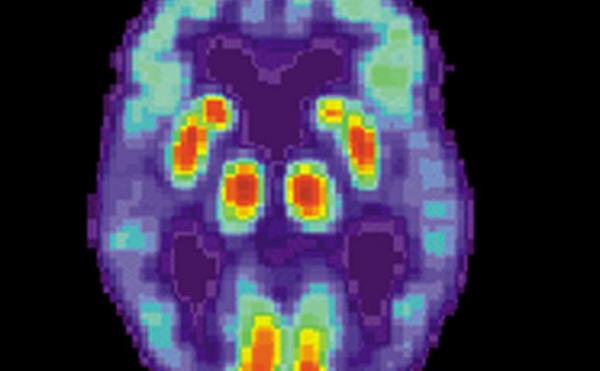
PET scan of a human brain with Alzheimer’s disease. Credit: public domain
A major new study on Alzheimer’s disease provides previously unknown evidence of how the brain-robbing illness may originate.
Moreover, it proposes that certain HIV drugs called reverse transcriptase inhibitors could immediately be repurposed for Alzheimer’s patients.
Led by scientists from Sanford Burnham Prebys Medical Discovery Institute in San Diego, the study finds that, as long suspected, Alzheimer’s is a genetic disease. But in nearly all cases, it’s not inherited. Rather, it arises during a patient’s lifetime by genetic rearrangements in neurons. Sequences of DNA are copied, altered and inserted back into the genome.
The genetic rearranging isn’t random mutation, but a process that recombines DNA into different patterns. This reshuffling creates a mosaic of slightly differing cells. The immune system uses a similar process to make antibodies, but nothing like it has been seen in the human brain.
Reverse transcriptase inhibitors might also ward off Alzheimer’s in those with Down syndrome, who develop Alzheimer’s as they age, the study said.
The study was published Wednesday in the journal Nature.
Confirmation of the findings is required, said Dr. Jerold Chun, the lead author. But Chun says testing with the HIV drugs should begin immediately. Even a low degree of effectiveness would be better than what is now available.
The study combines single and multiple-cell analytical methods to examine 13 donated human brains, some normal, some with Alzheimer’s. Its findings jibe with epidemiological data from elderly HIV patients. They have been treated with reverse transcriptase inhibitors for decades, and almost never get Alzheimer’s.
The first documented case of Alzheimer’s in an HIV-positive individual was reported in 2016.
Cautious praise for the study came from Dr. Paul Aisen, a longtime Alzheimer’s researcher who specializes in clinical trials. Aisen heads the University of Southern California Alzheimer’s Therapeutic Research Institute in San Diego.
“The authors carefully demonstrate that there are extensive modifications to genetic material in the Alzheimer’s disease brain,” Aisen said by email.
“These are changes that occur with aging, rather than inherited genetic characteristics. While this is an intriguing idea, the actual contribution of this age-related genetic change remains uncertain.”
Fred “Rusty” Gage, president of the Salk Institute and a noted brain expert, said the study’s results back up the claim that DNA sequences are copied and inserted back into the neuronal genome.
“These results are quite striking and could have implications for Alzheimer’s disease diagnosis and progression,” Gage said by email.
About 5.7 million Americans today have been diagnosed with Alzheimer’s disease, according to the Alzheimer’s Association. That number is expected to double by 2060, according to the Centers for Disease Control and Prevention.
In recent years, Alzheimer’s researchers have changed their view of the disease. They now say Alzheimer’s begins decades before symptoms appear. Eventually, the damage eating away at the brain becomes severe enough to affect cognition and memory.
So increasingly, researchers are looking for the earliest possible signs that Alzheimer’s is developing, before mental functions are affected.
The study traces the ultimate cause to the genetic rearrangements, so blocking this reshuffling should block Alzheimer’s.
The reshuffling can be likened to a copy-and-paste function in affected neurons. But instead of making an exact copy, the process scrambles DNA segments, then reinserts them back into the neuron’s genome.
Normal brains also show genetic variation in individual cells. Research suggests this condition is a normal part of brain development. Instead of having billions of identical neurons, each may vary slightly in a way that helps the brain work, Chun said.
This process goes wrong in producing the Alzheimer’s-causing variations, derived from a gene called APP. Certain variants of this gene are strongly linked with Alzheimer’s.
Because genes produce proteins, these rearrangements of the APP gene likely produce variations of toxic brain proteins called beta amyloid, known to be involved in Alzheimer’s.
Some of these genetic variants are found in a very rare form of Alzheimer’s that is directly inherited. Virtually all people with these variations come down with Alzheimer’s.
But this “familial” form constitutes only a few percent of all Alzheimer’s cases. The vast majority of “sporadic” Alzheimer’s cases shows genetic tendencies, but fall far short of a perfect correlation.
The study provides an explanation for sporadic Alzheimer’s: Because these genetic changes only occur in the brain, they don’t show up when a person’s genome is sequenced.
In addition, it may explain the failures of amyloid-based therapy. Billions of dollars have been spent developing drugs according to what is known as the “amyloid hypothesis,” with virtually nothing to show for it.
Chun said this may be because the amyloid drugs are aimed at a single molecular target, and there’s molecular diversity in amyloid.
“What our data strongly supports is that there could be many, many other targets that would have been missed by these single molecularly targeted therapeutics,” Chun said.
This means the amyloid hypothesis is essentially correct, but doesn’t go deep enough, Chun said.
In an accompanying perspective article, two University of California, San Diego Alzheimer’s researchers said the study was also important because it provided the “surprising existence” in the brain of what is called “somatic gene recombination.”
“This phenomenon, which has previously been reported only in antibody generation in immune cells, increases the diversity of proteins encoded by a given gene through DNA-shuffling mechanisms, wrote Guoliang Chai and Joseph G. Gleeson.
“The study hints at a previously unanticipated mechanism in the development of Alzheimer’s, and expands our understanding of the genesis of brain mosaicism,” they wrote. “But whether accumulation of (the recombined DNA) in neurons is a cause of or is caused by Alzheimer’s disease remains to be proved.”
Aisen cautioned that some studies indicate that Alzheimer’s is more likely linked to defects in removing amyloid, not their manufacture.
“So while there could be therapeutic implications of these new findings, additional clarification of this mechanism is needed,” Aisen said.
Doctors could use the HIV drugs on Alzheimer’s patients as an “off-label” use, Chun said. But that would require careful ethical consideration.
On the positive side, there’s no treatment now that affects the underlying neurodegeneration Alzheimer’s brings, and the safety profile of the HIV drugs is well-known.
“Let’s say this only works 25 percent of the time, that’s still 1.5 million patients in the United States, not to speak of their families,” he said.
And even a modest effect of preserving cognition for a few years would mean a great deal to those families, he said.
However, all drugs have risks, and Alzheimer’s patients tend to be elderly and may have other conditions.
Such off-label use also doesn’t provide a scientific basis for officially approving the drugs for Alzheimer’s. That’s the job of a properly designed clinical trial.
Designing such a trial will be complicated, Chun said. There’s the need to accurately find the patients who will likely benefit. Brain scans for amyloid deposits, which are now available, might help. But as for now, actual detection of the pathological brain mosaicism in living people isn’t possible.
The APP-linked variations spread with the help of an enzyme called reverse transcriptase that HIV uses to replicate, the study says.
With the help of reverse transcriptase, HIV copies its genome into the genome of infected cells. Since it becomes part of the cell’s DNA, HIV is very hard for the immune system to reach. Reverse transcriptase inhibitors, a regular part of HIV therapy, block this process.
Reverse transcriptase is also naturally found in the human body, and presumably plays an important function.
“Evolutionary biologists that have looked at the human genome, have estimated that nearly half of our genome was created by reverse transcription,” he said.
Whether HIV’s reverse transcriptase is identical to the human version isn’t known, Chun said.
Research funding was provided by The Shaffer Family Foundation; The Bruce Ford & Anne Smith Bundy Foundation; Sanford Burnham Prebys; the National Institutes of Health; and the government of Taiwan.
Wondering if having a second child will affect your marriage even more than baby number one did?
There’s no doubt that having a baby and changing from a couple into a family requires a lot of adjustment. But research shows that the adjustment period that follows a second child typically isn’t as long.
For most couples, the first month is the most challenging, but within four months, the quality of the marriage should be back to where it was before the second child arrived.
As with so many aspects of marriage, good communication is key. More important than the division of childcare responsibilities is clearly talking about who’s doing what, as well as working together to find solutions to problems that crop up. It also helps to have a network of support from family and friends.
Yet even couples who face a difficult transition and experience more disruption in their lives when they have a second child still return to their “pre-baby normal” by the fourth post-partum month, studies show.
Having navigated parenthood for the first time can give you the confidence you need to add to your family. And some advance planning for how you’ll manage after your second baby comes will ease the way to growing into a family of four.
Keep in mind that finding ways to handle the logistics of a new baby and helping your first child adjust to the new member of the family will also help ease the stress that both you and your spouse may feel during this time.
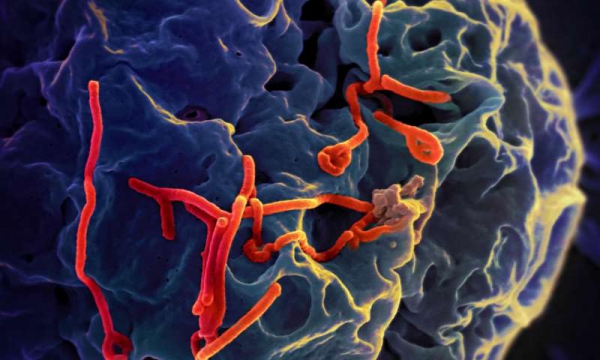
Ebola virus particles (red) on a larger cell. Credit: NIAID
The World Health Organization says a worrying number of the newest Ebola cases amid Congo’s ongoing outbreak are in patients not usually known to catch the disease: babies.
In an update published this week, the U.N. health agency reported 36 new confirmed cases of Ebola, including seven in newborn babies and infants younger than 2 years old. Six cases were reported in children aged between 2 and 17 and one case was in a pregnant woman.
While Ebola typically infects adults, as they are most likely to be exposed to the lethal virus, children have been known in some instances to catch the disease when they act as caregivers.
Few cases of Ebola in babies have been reported, but experts suspect transmission might happen via breast milk or close contact with infected parents. Ebola is typically spread by infected bodily fluids. WHO noted that health centers have been identified as a source of Ebola transmission, with injections of medications “a notable cause.”
WHO called Congo’s current epidemic “complex and challenging.” Congo’s health ministry says there are 346 confirmed cases, including 175 deaths, in what has become the worst Ebola outbreak in the country’s recorded history.
The outbreak has been plagued by security problems, with health workers attacked by rebels in districts where the virus has been spreading. Earlier this month, Ebola containment operations were paused after seven U.N. peacekeepers and 12 Congolese soldiers were killed, but all activities have resumed.
The increasing number of cases in children and health workers —39 health workers have been infected to date—suggests outbreak responders are having major problems stopping the virus in health clinics and convincing people to seek help when they develop symptoms. This is the first time this part of Congo has faced an Ebola outbreak.
WHO said the risk of the outbreak spreading to neighboring countries remains “very high” but it does not recommend travel restrictions. Uganda this month started vaccinating health workers against Ebola in a heavily traveled border district near the outbreak.
More than 8,200 women in England and Wales could have survived their heart attacks had they been given the same quality of treatment as men, according to new research.
The study did not include all hospital admissions which occurred over the 10-year study period so researchers say that the actual number of lives lost to unequal care is likely to be much higher.
Researchers from the University of Leeds used anonymised data from the UK’s national heart attack registry (MINAP) to analyse the treatment and outcomes of 691,290 people who were hospitalised for heart attack in England and Wales between 2003 and 2013.
The national registry included detailed information about each patient’s demographics, medical history and clinical characteristics such as heart rate when they entered hospital, and the investigations, treatments and procedures they received while in hospital.
In the British Heart Foundation (BHF) funded study, women tended to be older when admitted to hospital, and were more likely to have other illnesses such as diabetes and high blood pressure.
Even after adjusting for the fact that women who had a heart attack tended to be older and had more risk factors, the researchers found that women in the UK were more than twice as likely to die in the 30 days following a heart attack than men (5.2 per cent compared to 2.3 per cent). The researchers suggest that this may be, in part, explained by women being less likely to receive guideline recommended care.
Unequal care
Women who had a NSTEMI, a type of heart attack where the coronary artery is partially blocked, were 34 per cent less likely than men to receive a timely coronary angiography within 72 hours of their first symptoms (24.2 per cent of women compared to 36.7 per cent of men).
Coronary angiography creates video images to reveal narrowings or blockages in the coronary arteries. It’s a critical step in care because it helps doctors decide what to do next, and research shows that people who receive early angiography for NSTEMI have better outcomes as a result.
Women who had STEMI, a heart attack where the coronary artery is completely blocked, were 2.7 per cent less likely to receive timely reperfusion, emergency procedures including drugs and stents which help to clear blocked arteries and restore blood flow to the heart compared to men (76.8 per cent of women vs.78.9 per cent of men).
Women were 2.7 per cent less likely to be prescribed statins (87.6 per cent of women compared to 89.6 per cent of men) and 7.4 per cent less likely to be prescribed beta blockers (62.6 per cent of women compared to 67.6 per cent of men) when leaving hospital, drugs which help to lower their risk of having a second heart attack.
Although the difference in proportions may seem small in isolation, the researchers explain that even small deficits at each phase of a woman’s pathway of care can intensify into a considerable survival disadvantage.
Senior author Chris Gale, Professor of Cardiovascular Medicine at the University of Leeds and Honorary Consultant Cardiologist said: “We know women are dying due to unequal heart attack care – and now we’ve identified the shortfalls we need to target to save lives.
“For example, women not receiving coronary angiography when they arrive at hospital puts them at a disadvantage right from the start, and has knock-on effects creating further shortfalls down the line. In isolation the differences may appear small, but even in a high performing health system like the UK, small deficits in care across a population add up to reveal a much larger problem and a significant loss of life.
“We also show that not all differences are down to bias – some are down to biology. Only with more research can we hope to better understand how to target biology and best treat heart attacks in women.”
The researchers assessed the quality of care that men and women received following their heart attack based on ‘quality indicators’ – a checklist for the optimal care based on the international guidelines and endorsed by the European Society of Cardiology. Women’s care was less likely to meet 13 of the 16 heart attack quality indicators that were measured.
They estimated 8,243 deaths among women who were hospitalised with a heart attack in England and Wales could potentially have been prevented over the study period had they received care equal to that of men. But as the study did not include all heart attacks in the UK over the 10 year period, it is likely the true number of lives lost to unequal care is much higher.
The researchers point out that the differences in care likely explain much, but not all, of the gender gap in survival. Differences in heart attack symptoms, health-seeking behaviour, underlying biology, age and presence of underlying health problems, as well as response to drugs and treatments may have also played a role.
Each year in the UK around 70,000 women go to hospital due to a heart attack, and up to 25,000 women in the UK die each year from heart attacks – that’s three women every hour
Previous BHF-funded research has shown that women are 50 per cent more likely than men to receive the wrong initial diagnosis following a heart attack and are less likely to get a pre-hospital ECG, which is essential for swift diagnosis and treatment.
Professor Sir Nilesh Samani, Medical Director of the British Heart Foundation, said: “We need to tackle the false perception that heart attacks are only a male health issue. This leads to inadequate care for women – both at the time of and after heart attacks – with fatal consequences.
“While further research is needed, this study has identified several areas where heart attacks are being treated differently between the sexes, which may contribute to the worse outcomes in women. If we start to address these now, it will make a huge difference and save lives.”
Gut-directed hypnotherapy delivered by psychologists appears as effective in group or individual sessions, potentially offering a new treatment option for irritable bowel syndrome in primary and secondary care.
Hypnotherapy might help relieve irritable bowel syndrome (IBS) complaints for some patients for as long as 9 months after the end of treatment, according to a randomised controlled trial of 354 adults with IBS in primary and secondary care published in The Lancet Gastroenterology & Hepatology journal.
After 3 months of treatment, adequate relief of IBS symptoms was reported by more patients who received individual (40%; 41/102 for whom data were available) and group hypnotherapy (33%; 31/91) than those given education and supportive care (17%; 6/35), and these benefits persisted at 9 months follow-up (42% [38/91], 50% [40/80], and 22% [7/31]).
Importantly, the findings suggest that group hypnotherapy is as effective as individual sessions, which could enable many more patients with IBS to be treated at reduced cost.
The study is the largest randomised trial of hypnotherapy for IBS to date, and one of the first conducted in primary care, where the vast majority of IBS patients are treated.
The study found that IBS patients undergoing hypnotherapy reported a greater overall improvement in their condition and were more able to cope with, and were less troubled by, their symptoms compared with those who received educational supportive therapy. However, hypnotherapy did not appear to reduce the severity of symptoms.
While the findings are promising, the authors conclude that more research will be needed to test the optimum number of hypnotherapy sessions, the effect that patient expectations may have on treatment outcome, and the extent to which hypnotherapy outcomes are influenced by the magnitude of the psychological complaints of the patient.
“Our study indicates that hypnotherapy could be considered as a treatment option for patients with IBS, irrespective of symptom severity and IBS subtype,” says Dr. Carla Flik from the University Medical Center Utrecht, Netherlands, who led the research. “It is also promising to see that group hypnotherapy is as effective as individual sessions, which may mean that more people could be treated with it at lower cost, should it be confirmed in further studies.”
“What’s striking about these findings is the extent to which patient’s perception of their illness has an effect on their suffering, and that their perception of symptoms appears to be as important as actual symptom severity.”
IBS affects around 1 in 5 people worldwide and is a persistent and difficult-to-treat condition, with symptoms that can seriously affect quality of life including abdominal pain, bloating, diarrhoea, and constipation. For many sufferers, drug and dietary treatments are not successful.
Psychological interventions have proven effective, but their use is limited by a shortage of trained therapists. Hypnotherapy has previously shown promising results for IBS, but the majority of studies have been done in highly specialised centres, and more research is needed into whether hypnotherapy is beneficial in primary and secondary care where most patients are treated.
The IMAGINE study recruited 354 adults (aged 18-65 years) with IBS who were referred by primary care physicians and hospital specialists to 11 hospitals across the Netherlands between May 2011 and April 2016. Participants were randomly assigned to receive either 45-minute individual sessions (150 patients) or group sessions (150) of hypnotherapy twice weekly for 6 weeks, or education and supportive care (54).
Hypnotherapy treatment was provided by psychologists who were trained as hypnotherapists and involved a technique of positive visualisation during which patients were given suggestions about how they could gain control over their digestive system to reduce feelings of pain and discomfort. Patients were also given a CD so they could practice self-hypnosis exercises at home for 15-20 minutes every day.
Participants completed assessments on their level of symptom severity, quality of life, psychological symptoms, health-care costs, and work absence at the start of the trial and immediately after treatment (3 months) and again 9 months later, as well as symptom relief immediately after treatment and 9 months later.
Results showed that immediately after treatment, participants in the two hypnotherapy groups reported satisfactory relief at substantially higher rates than those who received educational supportive care, and these benefits persisted for 9 months after the treatment ended (table 2).
Nevertheless, satisfactory relief of symptoms was not accompanied by a significant improvement in symptom severity.
As Dr. Flik explains: “We do not know exactly how gut-directed hypnotherapy works, but it may change patients’ mindset and internal coping mechanisms, enabling them to increase their control over autonomic body processes, such as how they process pain and modulate gut activity.”
Improvements in quality of life, psychological complaints, cognitions and reductions in medical costs and IBS-related work absence were similar between groups.
Overall, hypnotherapy was well tolerated. Eight serious unexpected adverse reactions (six in the individual hypnotherapy group and two in the group hypnotherapy group) were reported, mostly cancer and inflammatory bowel disease, but were not related to hypnotherapy.
The authors note some limitations—for instance, that 22 (15%) patients in the individual hypnotherapy group, 22 (15%) in the group hypnotherapy group, and 11 (20%) in the control group dropped out before or during therapy, and a substantial number of participants did not complete questionnaires at 3 months and 9 months after treatment, which might have biased the results (figure 1). They also point out that the inexperience of therapists in dealing with IBS, and the low number (six) of hypnotherapy sessions provided (half the usual number), might have led to underestimations of the effects of hypnotherapy.
Writing in a linked Comment, Professor Olafur Palsson, University of North Carolina at Chapel Hill, USA discusses factors that may have contributed to the “modest” therapeutic impact of hypnosis in the study.
He writes: “The hypnotherapy tested in this study might have been suboptimal in amount or implementation. However, as the authors note, the smaller therapeutic effect in this trial compared with most hypnotherapy trials in tertiary care might have been because IBS in primary and secondary care is different to that in tertiary care—perhaps simpler in nature and with less involvement of psychological factors. Therefore, despite this impressive investigative effort by Flik and colleagues, it remains unclear whether gut-directed hypnotherapy is well suited for the treatment of patients with IBS in primary and secondary care, and future trials are needed to provide definitive answers.”
The gap between the life expectancy of the richest and poorest sectors of society in England is increasing, according to new research from Imperial College London.
The research, published in the journal Lancet Public Health, also reveals that the life expectancy of England’s poorest women has fallen since 2011, in what researchers say is a “deeply worrying” trend.
The study, funded by the Wellcome Trust, analysed Office for National Statistics data on all deaths recorded in England between 2001 and 2016—7.65 million deaths in total.
The results revealed the life expectancy gap between the most affluent and most deprived sectors of society increased from 6.1 years in 2001 to 7.9 years in 2016 for women, and from 9.0 to 9.7 years in men.
The life expectancy of women in the most deprived communities in 2016 was 78.8 years, compared to 86.7 years in the most affluent group. For men, the life expectancy was 74.0 years among the poorest, compared to 83.8 years among the richest.
The results also revealed that the life expectancy of women in the poorest sectors of society has dropped by 0.24 years since 2011.
Professor Majid Ezzati, senior author of the research from Imperial’s School of Public Health, said: “Falling life expectancy in the poorest communities is a deeply worrying indicator of the state of our nation’s health, and shows that we are leaving the most vulnerable out of the collective gain.
“We currently have a perfect storm of factors that can impact on health, and that are leading to poor people dying younger. Working income has stagnated and benefits have been cut, forcing many working families to use foodbanks. The price of healthy foods like fresh fruit and vegetables has increased relative to unhealthy, processed food, putting them out of the reach of the poorest.”
He added: “The funding squeeze for health and cuts to local government services since 2010 have also had a significant impact on the most deprived communities, leading to treatable diseases such as cancer being diagnosed too late, or people dying sooner from conditions like dementia.”
The research team also analysed the illnesses that contributed to the widening life expectancy gap. Although they found that people in the poorest sectors died at a higher rate from all illnesses, a number of diseases showed a particularly stark difference between rich and poor.
The diseases that led to particularly large loss of longevity in the poor compared to the rich were newborn deaths and children’s diseases, respiratory diseases, heart disease, lung and digestive cancers, and dementias. In 2016, children under five years old from the poorest sectors of society were 2.5 times as likely to die as children from affluent families.
“This study suggests the poor in England are dying from diseases that can be prevented and treated,” said Professor Ezzati. “Greater investment in health and social care in the most deprived areas will help reverse the worrying trends seen in our work. We also need government and industry action to eradicate food insecurity and make healthy food choices more affordable, so that the quality of a family’s diet isn’t dictated by their income.”
The team conducted their analysis by using information on the where each death occurred, which was matched to small areas of England known as lower super output areas by the Office of National Statistics. These lower super output areas, which each have a population of around 1,500 people, are given a score of deprivation from the Office of National Statistics (called an Index of Multiple Deprivation). The research team point out this means the comparisons are based on a community’s deprivation and affluence, and not that of individuals.
Reliance on carers makes nursing home residents especially vulnerable to sex abuse. Credit: shutterstock.com
We don’t often think of older women being victims of sexual assault, but such assaults occur in many settings and circumstances, including in nursing homes. Our research, published this week in the journal Legal Medicine, analysed 28 forensic medical examinations of female nursing home residents who had allegedly been victims of sexual assault in Victoria over a 15-year period.
The cases were examined by Clinical Forensic Medicine – a division of the Victorian Institute of Forensic Medicine – between January 1, 2000 and December 31, 2015.
The majority of the alleged victims had some form of cognitive or physical impairment. All 14 perpetrators who were reported were male, half of whom were staff and half other residents. The majority of case reports didn’t indicate whether the alleged victim had received treatment for the assault.
The most frequent alleged sexual contact was vaginal contact or penetration. Injuries weren’t reported for every case. Where present, they consisted of bruising, skin tears, redness and swelling.
The physical examination was often limited because of the cognitive status (in 38%) of the individuals, physical issues (in 31%), lack of cooperation (23%), and poor examination conditions (23%). Data on alleged victims’ behaviour was commonly missing.
These information gaps highlight the difficulty of examination which is essential to a detailed investigation. A better understanding of the context and setting of the assault, which is usually available when younger women are victims, is essential to inform prevention efforts.
Eliminating sexual assault in nursing homes is a major challenge which starts with acknowledging it exists and recognising the scale of this abuse.
Much higher than we think
Sexual assault is considered the most hidden, as well as least acknowledged and reported, form of elder abuse. This makes it difficult to accurately estimate its prevalence.
Prior to 2007, it was estimated there were around 20,000 unreported cases of elder abuse, neglect and exploitation in Victoria. Between 2009-10 and 2014-2015 the published number of sexual assaults among older people rose from around 280 to 430 reports nationally (information about each jurisdiction was not available).
In 2015–2016 The Australian Department of Health was notified of 396 reports of alleged or suspected unlawful sexual contact of residents in nursing homes in Australia.
Based on these statistics, we expected Victoria would have 80-120 sexual assaults of residents reported in nursing homes per year (equating to approximately 1,200 assaults during the study period). The 28 cases reported to the forensic investigation team over a 15 year period suggests under-recognition and under-reporting.
Nursing home residents are particularly vulnerable to sexual assault due to their dependency on caregivers, health problems, and the co-housing of residents, sometimes with potentially dangerous older individuals with sexual assault backgrounds.
Negative stereotypes such as that older people aren’t sexual beings, their greater dependency on others, potential divided loyalty to staff members or residents are unique barriers to reporting, detecting, and preventing sexual assault in nursing homes. Despite severe health consequences, efforts to prevent and address elder abuse remain inadequate.
In the majority of cases we examined, signs of general or genital injury were not found. Further, post-assault victim responses, such as agitation, distress and confusion may mirror symptoms of cognitive impairment. This can create difficulties for nursing home staff in distinguishing between the usual behaviour or a response to trauma, such as sexual assault.
Also, nursing home victims of sexual assault tend to be ignored by staff who often don’t believe the accusations. Although we could not determine who or what prompted reporting, what is known is that sexual assaults are unlikely to have a witness, though witnesses appear to be crucial to ensure successful prosecution.
Sexual assault, in any setting or age group, is one of the most difficult crimes to prosecute due to the required elements of intent and lack of consent. But this is made all the more complicated when it comes to nursing home residents.
Awareness is crucial
Staff must be aware of the existence of sexual assault in nursing homes. It is their duty as care providers to report alleged or suspected sexual assault in a timely manner. More education, training and research is needed to address the knowledge gaps around incidence, levels of reporting, nature of investigations, responses required to better assist the victim, and the interventions needed to prevent sexual assault.
Without a clear understanding of the alleged victim and incident characteristics, we will struggle to combat sexual assaults in nursing homes. There is an urgent need to better use the existing data held by the the Department of Health to understand the full extent of sexual assault in nursing homes. The Royal Commission is an opportunity to consider the development of tailored policies, staff training and legislation.
An international study lead by University of Manchester scientists has discovered the identity of genes that predispose people to chronic kidney disease.
The discovery is a major advance in understanding of the significantly under-diagnosed disorder which, if left undetected, can lead to failing kidneys that need dialysis or kidney transplantation.
The discovery of 35 kidney genes is an important step forward to the future development of new diagnostic tests and treatments for the disease that affects around one in ten adults.
The team, based in Poland, Australia and the UK publish the Kidney Research UK funded study in Nature Communications today.
Lead researcher Professor Maciej Tomaszewski from The University of Manchester said: “Chronic kidney disease is known for its strong genetic component.
“Our limited knowledge of its exact genetic mechanisms partly explains why progress in the development of new diagnostic tests and treatments of chronic kidney disease has been so slow.
“The findings were made possible by using a state-of-the art technology known as “next-generation RNA sequencing” applied to one of the largest ever collections of human kidneys.
“We hope that some of the kidney genes we discovered may become attractive targets for the development of future diagnostics and treatment for patients with chronic kidney disease.”
Co-author Professor Adrian Woolf from Manchester Children’s Hospital and The Universality of Manchester said: “One of the genes—mucin-1- is especially interesting.
“It makes a sticky protein called mucin that coats urinary tubes inside the kidney. Mutations of this gene have already been found in rare families with inherited kidney failure”
Professor Fadi Charchar from Federation University Australia said: “We hope that early prediction by genetic testing even before the development of symptoms will in the future be the first line of defence against one of the world’s top killers.”
“Early detection followed by treatment using kidney-protective medication or avoidance of drugs which can damage the kidneys is the key to healthier kidneys later in life.”
Director of research operations at Kidney Research UK, Elaine Davies said: “Nearly 2 million people in the UK have been diagnosed with moderate-severe CKD by their GP but it is estimated that a further one million people remain undiagnosed. We refer to CKD as a silent killer because it is common for it to have little or no symptoms until the consequences of the disease have taken hold.
“The findings of this research are hugely important as they bring us a step closer to being able to understand, diagnose earlier and prevent kidney disease.”
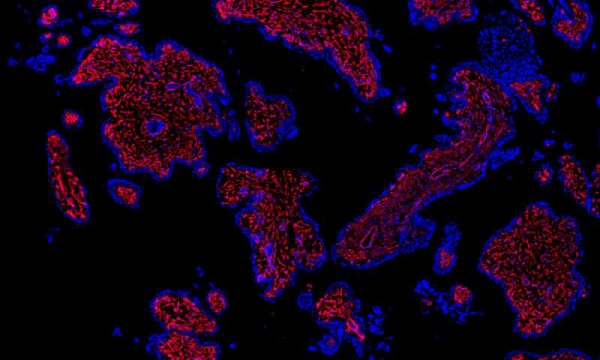
Researchers have mapped more than 20 different cell types present in the first-trimester human placenta, including stromal and endothelial cells (red). Credit: Rockefeller University
To treat and prevent pregnancy-related disorders, researchers must understand not only what can go wrong, but when. Complications, such as preeclampsia and pre-term birth, often occur in the second or third trimester, and most research to date has focused on those later stages of pregnancy. But the biological events that lead to these problems could start much earlier.
In a new Rockefeller study, published in Science Advances, scientists present the first detailed descriptions of both fetal and maternal cells that are present during the first trimester, a body of work they say could inform further research into a variety of pregnancy complications.
Parent and child, cells and genes
The researchers analyzed cells from placental and decidual, or endometrial, tissues, which allowed them to look at cellular features in the fetus and mother, respectively. In their samples they identified 20 distinct cell types—nine from the placenta and eleven from the decidua.
“It’s the first cellular atlas of the early human placenta,” says Hemant Suryawanshi, first author on the paper and a postdoctoral associate in the lab of Thomas Tuschl.
In addition to identifying different cell types, the scientists used a novel method to determine which genes were expressed by each of those cells. Previous research on first trimester tissue, explains Suryawanshi, relied on a method called bulk RNA sequencing, which generates averaged RNA profile from multiple cells, rather than specific data derived from single cells.
For this study, by contrast, Suryawanshi and colleagues used a microfluidics based single-cell RNA sequencing method to analyze more than 14,000 individual placental cells and nearly 7,000 individual decidual cells, all from first trimester tissue. No previous single-cell RNA study had looked at more than two dozens decidual cells, Suryawanshi says, and those cells were from second and third trimester tissue.
“We now have a profile for the many thousands of genes expressed by each of the 20 cell types,” he says.
Solving maternity mysteries
The atlas, says Suryawanshi, could become a useful tool for future researchers. For example, a scientist interested in first-trimester endometrial epithelial cells, which are found in the decidua and play a crucial role during embryonic implantation, could use it to see which genes those cells express, as well as the “strength of expression” of each gene, data which the new paper includes.
The need for such a tool is clear, says Zev Williams, chief of Reproductive Endocrinology and Infertility at Columbia University Medical Center, who contributed to the study. “The placenta is a profoundly important yet poorly understood organ. It is essential for life and, for our time in the uterus, functions as the lungs, kidney, liver and immune system. Yet, its structure and function are still very much a mystery.”
Part of that mystery involves the interaction between the fetus and mother during the first trimester. “Why doesn’t the mother’s immune system, as it normally would, reject the fetus, which in many ways is analogous to an organ transplant or a parasite invasion?” asks Suryawanshi.
The answer may lie in the cellular communication between the placenta and the decidua wall, which sheds off when there is no implantation.
“In the presence of pregnancy, there are dramatic changes in cellular composition and at the molecular level. Now, for the first time, we have high-resolution pictures of those changes,” he says.
And, because the atlas is a blueprint of normal first-trimester tissue and cell types, it could potentially serve as a template to help identify abnormalities at the cellular and genetic level in problem pregnancies.
“We can now begin to understand how the placenta and decidua work in concert to enable healthy pregnancies to occur,” says Williams. “By understanding, in detail, the diversity and specialized functions of cells that comprise the early placenta and the decidua, we can start to discover the underlying causes of many diseases of pregnancy and, ultimately, develop ways to improve pregnancy outcomes.”